


By Lori Passarelli, ABO-AC
According to The American Board of Optometry, Americans are on their computers and other electronic devices more than ever before—an average of 7 hours a day—and it's causing an unprecedented amount of eye-related symptoms. Clinicians commonly refer this to as Digital Vision Syndrome (DVS), or Computer Vision Syndrome (CVS), with headaches, dry eyes, neck pain, and eyestrain or asthenopia being some common complaints. An estimated 50-90% of adults who work on computers and children who stare at tablets or other devices report symptoms of DVS.
For years, the most commonly attributed factors to DVS included the poorly defined print on electronic devices compared to print on paper and the glare emitting from digital screens, which causes reflections, glare, and flickers. As such, the typical remedy to reduce symptoms of DVS encourages the patient to use the 20-20-20 rule and wear corrective lenses with a blue light filter. However, recent research suggests that fusion problems during near convergence fixation without a double vision malady leads to symptoms of DVS. These binocular vision disorders are non-strabismic and cannot be corrected by lenses with a mere blue light filter.
A lot goes into keeping the eyes aligned; our eyes must constantly re-adjust and focus as we scan the screen. Six muscles control each eye. Two extraocular muscles, the medial rectus, and lateral rectus control horizontal movements by constantly alternating contraction and relaxation—four muscles per eye control vertical balance. When we consider that our eyes move about 240 times a minute, it's easy to appreciate the workout our eye muscles get every day. Not only are our eye muscles in constant movement, but our visual system also interprets countless images throughout the day and reconciles information from both peripheral with central vision. It is not surprising, then, that undetectable subtle eye misalignments, or phorias, missed by standard cover tests, may also play a role in symptoms associated with DVS, as eye muscles struggle to keep the eyes aligned during convergence. These subtle undetected phorias are typically overlooked and unaddressed or uncorrected and may cause DVS symptoms by inducing trigeminal dysphoria.
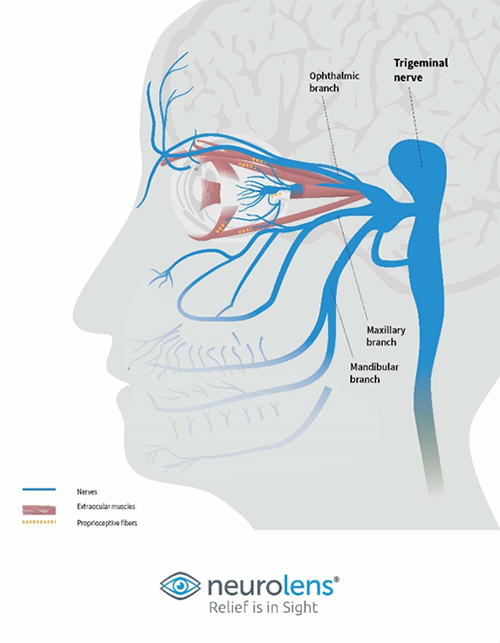 |
| Figure 1 Trigeminal Nerve |
The Trigeminal nerve (Fig.1) is the fifth cranial nerve, with one of its three branches innervating the eye. The ophthalmic branch of the trigeminal nerve carries sensory signals to the brainstem. It, too, has three branches: the frontal nerve, the lacrimal nerve, and the nasociliary nerve. These three nerve branches provide sensory nervation to the conjunctiva, upper eyelids, lacrimal glands, cornea, and pupil.
With the eyes' constant realignment of central and peripheral vision, the extraocular muscles' proprioceptive fiber signals travel the trigeminal nerve's eye-related branch, overstimulating it and causing symptoms associated with DVS. Although double vision may not be a reported symptom of digital eye strain, small undetectable amounts of diplopia likely occur.
Typically, phorias cause diplopia or double vision and are correctable with a prism in glasses. But small, nearly undetectable amounts of prism to correct non-diplopic phorias would require a customized placement and small incremental amounts of prism unavailable in standard optical lenses. Neurolens solves the problem by incorporating a contoured prism into its lens designs, placing the prism correction where it’s needed most—as well as offering a device that can detect eye misalignment as small as 0.01 prism diopters.
 |
| Figure 2 Neurolens Measurement Device Gen 2 NMD2 |
The NMD2 is easy to use and results in accurate, non-subjective measurements. The test takes about two minutes and can be easily administered by a technician. Doctors prescribe Neurolens with precise contoured prism lenses using the measurements gained by the device, thereby relieving patients of DVS symptoms, and achieving clear, crisp and a comfortable binocular fusion. Watch the interview with Dr. Sudarsky and optician Jordan Park in Pro to Pro Perspectives video.









