


The 2006 Tech for Success details two new sections this year. In “Pre Testing and Refraction,” a variety of software, hardware and skills needed are covered. As in all successful practices, they combine the knowledge and personal warmth of doctor and staff with highly sophisticated technologies to deliver the gold standard in patient care.These new technologies touch every portion of the patient care process and can assist the doctor and staff to better meet each patient’s individual need. However, it’s often difficult to understand and determine what technology fits best in which part of the office. Therefore, Jobson Medical Information and 20/20 magazine have compiled a review of technologies to assist in the decision. This guide provides background, benchmarks and details of how technology can improve patient care and satisfaction, practice efficiency, profitable growth as well as enhance a professional identity. In a simple format it discusses the goals, skills, hardware, software, implementation and followup required that makes an infusion of new technologies seamless to any practice. Whether your office requires a step change in capability or there is a need to improve specific practice areas, this guide will allow optometrist, ophthalmologist or optician to learn about new devices and techniques in a variety of business and practice areas. Areas Highlighted in this IssueSome technologies are designed to touch all aspects of a practice, some only one, some are entry level, others highly complex, so to best determine what technology belongs in your office, we’ve created a roadmap of a patient’s visit to review what could happen at each step. The areas in this technology review are: From Reception to EyewearTo capture a patient’s loyalty, everyone in the office needs to help the patient understand the benefits of good eye health and the best in vision solutions. The receptionist is the first point of contact to talk in general about the office and its staff, what happens during an appointment, the variety of tests and the products patients will learn about when visiting. The reception area (it’s not a waiting room) should be used to teach and predispose patients about choices. So, the reception area is the perfect place to install technology since it is the first impression that each patient experiences. A handheld computer delivering new product and eye health information improves a patient’s awareness of their options. It allows for a better exam also since the patient will be reminded to tell about their all eyewear needs. 
WinkPad is a handheld educational interactive touch screen given to the patient while waiting in reception. The device contains a color screen and speakers (or headphones) and responds to the touch of a finger. It is confidential, personalized, fun and simple to use. WinkPad anonymously questions patients about their optical needs and preferences, and then customizes a series of information screens based on their answers. It educates patients on premium products, is sponsored by major optical companies but is focused on education. The educational media is produced by Jobson Internet Solutions and is available from Wink Interactive, Inc. The technician initiates the exam, records history and collects field, corneal, auto refractor and retinal image data. This is an opportunity to answer patient’s questions about their vision test and the needs that the doctor can address. Here the patient begins their travels through the variety of modern technologies in the office.
The optician continues to use technology in measurement devices and the new technologies embedded in lenses in their designs, materials and treatments. When consumers understand the benefits of new technologies, they are more apt to consider and value a recommendation to buy. Technology helps the practitioner to more competently measure and examine, the technician to get better data and the optician to clearly demonstrate the benefits available in new products to better meet a patient’s health and vision needs. Take the time to consider the ideas and products described in this book, see them at trade shows and buy the best tools that you can afford to better grow your practice. The Office System BackboneThe goals of an office system backbone is to efficiently provide improved patient care and easily mine the data collected so that a practice can be managed to the details of the business and profession. Today, this is easier than ever because the complexity of the practice can be made simpler through management with software. However, the choice of the right software can appear daunting since the number of operations within an office today has increased complexity and the relationship with outside suppliers and third party providers all appear different. Therefore, how does one make a choice whether it’s the first system of a new practice or a significant upgrade to an existing system? There are a number of software firms to choose from that specialize in practice management software so having a list of critical components that are prioritized is important. Bill Hatch of OfficeMate suggests that the simpler and easier the system is to navigate, the easier it will be to implement. In fact, that priority will also drive the implementation schedule. For example, we previously covered the opportunities that great presentation graphics for patient and product education provide throughout the patient experience in the office. Products like iPoint gives eyecare professionals an end-to-end solution from the front office, pretest and exam rooms, business office, and optical dispensary. Virtual Try On technology gives dispensers and professionals an effective way to present frame selection options, lens enhancements, and color contact lens simulations in a patient friendly way. Practice websites deliver visibility and patient education, allow patient own scheduling or provide a place to order product replacements like contacts. Regardless of the need, having a web site has become a requirement in an environment that demands information 24/7. Software management tools that can create websites using templated choice are simple for the office to set up. Eyecarepro.net, Eyefinity as well as other practice management software’s allow website creation. Web building features can be affordable and give practitioners a seamless and powerful productivity tool. For example, in Eyecarepro. net, patients can complete history forms online and have the data integrated into OfficeMate on the practice’s desktop. Imagine the time savings for staff, if a patient can also do their own scheduling in real-time online. Look for these features when choosing the backbone of the office. Resource Contact Information Patient History and Pre-testingBy Rebecca L. Johnson, CPOT, COT, COE GoalsA clear patient history allows the practitioner to best determine current eye health and ensure that future health needs are considered. If there is a complete history of the patient’s complaints, previous and current eyewear and their impression of their needs, the office is best prepared to provide a comprehensive exam that answers eye heath and eye care wants. Obtaining patient history and performing pre-testing are critical parts of the ophthalmic examination and are usually conducted by an ophthalmic technician. Because the information gathered in both of these exam components is vital, staff training is required and staff retention should be the goal of any office. Hiring and training a new technician is time-consuming and costly. Improvements in technology have eliminated some of the training issues with “focus, point and click” testing and formatted electronic medical records. Much of modern ophthalmic instrumentation requires the operator to be computer savvy and comfortable with advances in technology. So, take this into consideration during the technician hiring process. What improvements to instrumentation and software can affect the efficiency and professionalism of any office? Electronic Medical RecordsThe addition of electronic medical records has brought consistency and efficiency to the clinic. Increased clinic efficiency equals increased quality time with the patient, increased patient satisfaction, increased profits, and decrease in costs. Many EMR programs incorporate a patient-tracking module to make the flow of patients more efficient. Sally Crowell of Crowell Systems says, “Manually, it is very difficult to be certain that the flow of patients through the practice is efficient and that each task is done at the appropriate time. The Practice Traffic Controller (PTC) solves that problem. The PTC eliminates flags and lighted call buttons. It tracks all patients as they check in. They are put in different statuses—workup, doctor, testing, dilation, optical, check out—as they move from room to room. Doctors can create work orders on an individual patient basis that direct the staff to perform special testing. This ability allows the patient to be handed off to the correct person at the right time. It eliminates the confusion of wondering what needs to be done for each patient and allows the doctor to use time more efficiently without diminishing the quality of patient care. Another advantage of the PTC is that it enables Medformix to record the amount of time spent in each status and the total time for each visit. This feature is extremely helpful when handling any patient complaints. It reveals bottlenecks in the work flow so that management can make any necessary adjustments.” Organization of information is crucial in patient charting. EMR has taken charting to the next level by allowing specific information requests. For example, if the doctor wishes to view only intraocular pressures changes over a period of time, the software will sort out and display only the IOP measurements. The ExamWRITER by OfficeMate converts the IOP measurements into a graph for quick analyzing. The test tracking module of Compulink provides an area to view tests (such as OCT, HRT, lab work, MRIs, etc.) that have been ordered and documents when they have been reviewed. Insurance companies mandate key components in areas of history and pre-testing. Most EMR software manufacturers attempt to insure that all insurance components are included in the documentation by incorporation of forced-entry fields. They alert the doctor and staff to incomplete areas of documentation; some programs suggest a CPT code based on exam documentation. “The Medformix Medical Module has been designed and refined by our client doctors over the past 23 years,” says Crowell. “As findings are entered, Chartscore creates a graph indicating the components of the exam that are documented, as well as those where no documentation exists. In my experience of working with numerous doctors, they often are uncertain of the correct level of service to bill. Due to uncertainty or fear, they often under-code and short themselves quite a bit of deserved revenue. Medformix with Chartscore solves that problem.” Rachel Mandac of Compulink notes, “Eyecare Advantage includes automated coding for the medical Evaluation and Management codes with the ability to assign cross-over codes for the ‘92’ codes by plan.” Ian Lane, OD of OfficeMate says, “ExamWRITER lays the documentation in the correct format. The system walks through documenting Chief Complaint, HPI (History of Present Illness) and ROS (Review of Systems) to assure compliance with guidelines. In addition Exam- WRITER contains a feature that counts all the elements documented and compares this to the E/M code to assure compliance.” (See ExamWRITER) Practice Director, a new software product by Williams Group, also incorporates a module that scores the exam. John Lee of Practice Director says, “Practice Director is a practice productivity and electronic health record software system. Practicing optometrists designed it with input from Dr. Chuck Brownlow, a frequent speaker on the national circuit regarding proper medical record keeping and coding. The software includes all the checks and balances necessary to code at the appropriate level using the E&M coding guidelines. For instance, the electronic health record scores the exam factoring in the history of present illness, past family and social history, review of systems, case history, physical exam, diagnosis, risk, medical decision making, and face to face time with the patient to generate the appropriate coding level.”
Chart unavailability also decreases clinic efficiency. Creating a temporary chart takes time and can cause the patient to lose confidence in the doctor. EMR software allows access to the medical record at all satellite locations at the press of a button. Access to the records from home makes after-hours calls much easier to manage. Communicating eye glass needs to the optician can be done very effectively with EMR. “After recording a complete exam, there has always been a potential for a loss of communication of the doctors instructions to the optical staff. ExamWRITER allows the doctor to write a complete lab order right on the final spectacle screen. This lab order will include RX, lab order options, special instructions, Rx notes and any observations. This is one significant key to completing the total paperless office solution,” says Gregg Seacrist of OfficeMate. An EMR software program should integrate with pre-testing equipment so that the information from the test is automatically pulled into the medical record. “Compulink has established relationships with Marco, Topcon and Carl Zeiss Meditec to shuttle information from testing equipment directly into the Compulink Electronic Health Record,” says Mandac. The early years of electronic medical records were less than successful, somewhat due to the cumbersome training process. Today, very few individuals lack the basic computer skills required to learn EMR software. “Compulink provides on-site training, web-based training and on-going WebEx classes to assist with product enhancements and also orientation for new staff,” says Mandac. “The Medformix charting system leads the technician through their portions of the exam. After a few days, the technician is able to fly through their work as data entry takes much less time than handwriting a chart,” notes Crowell. “The average technician requires about four hours of training and traditionally is more productive within a few days of ‘going live’ with Exam- WRITER,” says Dr. Lane. “Practice Director includes online modules followed by user certification. After user certification, the office staff can play with the software using actual patient date in “sandbox” or practice mode for several weeks before going live on the system. This gives the staff plenty of time to learn the software and use it in practice mode before depending on it every day,” says Lee. Pre-TestingVisual Acuity: Screening systems
Testing visual acuity does not always provide the patient’s real-world vision capabilities. The Functional Vision Analyzer (Stereo Optical Co., Inc.) provides options to stimulate various environmental factors, including day/night with and without glare. Images of non-corrected and corrected vision can be demonstrated to the patient. When the Functional Vision Analyzer is teamed with EyeView Software, the practitioner has access to instant F.A.C.T. and EDTRS test scores, report graphs and summaries, including contrast sensitivity curve and the ability to display pictorial images that compare the results side-by-side with a normal vision image. Lensometry This technology allows the lensmeter to simultaneously measure 108 multiple points for greater consistency and reliability. This same lensmeter has a prism range of 20 diopters and UV assessment. Auto-refraction/Auto-keratometry
Auto-refractors have historically taken up a large area of square footage in the clinic. Over the past 5 years, advancing technology has allowed for the design of portable, hand-held auto-refractors and auto-keratometers. The Palm- ARK handheld (Marco) can accurately measure sphere power up to -/+ 20 D and cylinder powers up to -/+12.00D. Perimetry Sandra Mohring, of Haag-Streit USA says, “The Octopus 311 Perimeter offers three methods on one instrument: standard static white/white and both blue/yellow and flicker perimetry for early detection of glaucoma. Standard thresholds are completed in only 2-1/2 minutes per eye—much faster than the older days of 12 to 20 minutes. A more comfortable patient is a more accurate field. All perimeters provide 100 percent fixation control—you never need to worry about fixation losses. In addition, the 300 series provides an automatic eye tracking system that allows for a stationary chin rest. We move the instrument—not the patient. This allows for the patient to continue focusing and not be interrupted.” When discussing new perimeter technology, one must include the Welch Allen Frequency Doubling Technology found in the Humphrey FTD Perimeter. An excellent glaucoma screening device, it can perform supra-threshold testing in only 35 seconds. Full threshold testing, complete with statistical analysis can be achieved in four minutes (see www.meditec. zeiss.com). The perimeter, which is compact and lightweight (19 pounds), can easily be moved from room to room or clinic to clinic. Tonometry Retinal ImagingNon-Mydriatic Retinal Camera “Second, look for owner upgradeability. If the retinal camera has a CCD chip trapped inside the camera you won’t be able to upgrade the mega pixels in the future. If the cameras computer is built in, or proprietary—plan on spending big bucks when it comes time to upgrade. “Most Non-Mydriatic cameras will last 10 to 20 years. In that length of time it won’t be uncommon to replace the computer four or five times and the digital back two or three. Make sure your camera comes with software that you can simply add to any computer that you purchase in the future. Ask if the data can be migrated to a new computer and if there is any charge for doing so. Also make sure you can upgrade the resolution of the camera as technology changes. You don’t want to be stuck with a 5 mega pixel retinal camera when the standard becomes 30 or 40 mega pixels. Avoid cameras with built in obsolescence. “Finally, look at the images. It is easy to walk the aisles of a trade show and make the killer deal only to learn after the camera is installed that diabetic bleeders you see in the slit lamp aren’t on the retinal photos because your camera adds red, orange or brown tones to every image. It’s also frustrating to learn that you can’t photograph a nerve head hemorrhage because your camera blows-out nerve head images. Know the clinical limitations.” Glen Barnes of Sunshine Ophthalmic, L.L.C. adds, “There are several good systems in the market today; the ability to have a modular system is the key. The ability to upgrade the capture system (the camera back) is very important, as this allows the doctor to upgrade the camera back as technology improves without having to replace the entire system.” When asked about new technology, Whalen says, “Synemed provides the latest computers in the way of speed, RAM, storage capacity, and networking capability. We’ve also adapted the latest Canon EOS digital backs to the Synemed packages. For example, we have gone from two to a standard configuration of 8.2 mega pixels with optional packages of 13 and 16 mega pixels. “The EyeScape Digital Imaging Solutions Software has evolved as well. Currently there is single click access to virtually all modes and functions, roller zoom, seven color tracks for clinical viewing, dedicated stereo pairing and storage, and much more. The system also interfaces with most EMR software programs. “Synemed has recently introduced two new modules to the EyeScape System. First, the StereoPlus Glaucoma Module is a separate program that allows for dedicated viewing of stereographic photos. The StereoPlus module allows for careful marking of the rim and disc under stereo observation. After marking, these drawings are converted into graphs that can be viewed. These graphs can be used for intra and inter eye comparisons over time. Second, The EyeScreen Wellness and Screening Module allows for screening photos of their patients without interfering with the ability to bill pathology photos.” The optomap Retinal Exam Practitioners can educate patients about retinal structures and explain treatment options for conditions such as diabetic retinopathy and macular degeneration. The visual impact also improves patient compliance. Showing patients the subtle changes in their eye tissue can help motivate patients to abide by health regimens that protect their sight.” Optos offers on-site staff training, along with materials to educate patients about the benefits of the optomap Retinal Exam. Scanning Laser Polarimetry, GDx This change is called retardation and is then detected by an analyzer. The amount of retardation from the RNFL is directly proportional to RNL thickness. Isabella Crawford of Carl Zeiss Meditec, Inc. says, “The GDx from Carl Zeiss Meditec provides highly detailed and reproducible RNFL analysis of a 20° x 20° area around the optic disc. It compares measurements to a large, multi-racial normative database and has been shown to predict visual field loss. In addition, the instrument has a unique ‘screening mode’ to help assess which patients require a full glaucoma workup. Scans are easy to perform, do not require dilation, and take between one and three minutes. Operators can be trained in a short time, and results are operator independent, which is especially important for analyzing change over time. It is also easily portable for use in multiple offices. These features make it an ideal diagnostic and management tool for glaucoma specialists as well as those building a glaucoma practice.” Heidelberg Retina Tomograph (HRT) good utilization of space and personnel. Travis Lindsay of Heidelberg Engineering says, “Although the technology for the Heidelberg Retina Tomograph (HRT) has been around for over 15 years, it is only in the last couple of years that the results from long term clinical trials confirm the predictive value of the HRT in glaucoma, most recently from the NEI-sponsored Ocular Hypertension Treatment Study (OHTS). Now the question is; is it time to throw away visual fields? Most say probably not. The OHTS results showed that glaucoma was first detected in 55 percent of patients by optic disc assessment, but visual fields detected damage first in 35 percent of patients. The jury is still out, but it may be tipping in favor of imaging. The 3D image feeds back precise measurements of the cup, rim and RNFL with classifications, which may point to early glaucoma in suspected cases. Leo Semes, OD of the University of Alabama at Birmingham is impressed with the results of HRT technology. “The HRT technology has created a new view of the optic nerve in many ways” he says. “First, the innovative presentation of images allows the practitioner to analyze data in a more careful and objective way. Second, it allows observation of following structural change objectively. The change analysis (GPS) offers the practitioner in the ability to monitor minute changes or trends in progression. This new method in optic nerve analysis offers an additional clinical dimension for both diagnosis and progression analysis. For patient care, it allows the practitioner to demonstrate, using printouts, the data collected and why the practitioner’s recommendation is what it is. Conveying these to the patient would support the practitioner’s recommendations. “Training is specific and detailed but minimal for any technician with a background in ophthalmics. The understanding of the instrument is straightforward. Obtaining the orientation and centration for data collection is easy with minimal practice.” In September 2006, Heidelberg Engineering unveiled new software to map both retinal thickness and an Edema Index of the macula. (See Thickness Map) “These two tools may turn out to be one of the earliest indicators of diabetic macular edema. And with a dramatic increase in obesity in the U.S., optometry may become the front line for detecting diabetes,” says Lindsay.
RefractionAutomated Refraction Systems The refracting systems interface with the majority of electronic medical record (EMR) software, allowing the current prescription, auto refraction, keratometry and manifest refraction to appear seamlessly within the medical record and a potential for increase in optical sales. “Topcon’s CV- 5000 includes patient education tools that give the patient the opportunity to evaluate simulated images while looking through a variety of single and multifocal lenses,” says Stephen Hamilton of Topcon. Marco’s Epic 5100 can be integrated with the 3D Wave, which measures and displays the changes in vision from day to night. This allows the doctor to show patients who complain of night glare and halos how the vision would improve with night driving glasses. Implementation The Future of Refraction and Vision Correction Wavefront Technology Conventional refractometry can evaluate two types of refractive error: spherical and cylindrical. The use of wavefront technology allows detection of ocular aberrations by shining a laser light into the pupil. The light reflected from the retina back through the pupil is distorted by the refractive properties in the eye, creating a “map” of the refractive error of the eye. This technology has been utilized primarily with laser vision correction. In late 2005, Ophthonix Incorporated (San Diego), announced the availability of a spectacle lens that has been adjusted using the results of a wavefront analysis of the eye. The technology of altering lens performance is called the iZon lens. Ophthonix markets this lens as a “High Resolution Lens” that provides the high-definition benefits of richer color, greater contrast and depth perception and improved nighttime driving reaction time. The iZon lens includes high index material (1.6), along with its proprietary anti-reflective and scratch-resistant coating. It is now available in single vision and progressive designs. To prescribe this lens, an instrument known as the Ophthonix Z-View Aberrometer must be used. This instrument takes wavefront measurements of the eye to create a unique optical fingerprint (iPrint) that is used to customize the lens. Your Role in Refractive SurgeryRefractive Surgery Options Stephen E. Smith, MD of Fort Myers Eye Associates adds, “The buzz word in laser refractive surgery is “iris registration.” This deals with the laser’s ability to track the eye during the procedure. In-office Procedures—A Role and Opportunity for Specialized Technicians Staff Skills and Training A technician who works with refractive patients should be a detail-orientated person with a positive, upbeat attitude and excellent communication skills. The refractive patient can require additional “handholding” as he or she is making a significant financial investment to be free of glasses and/or contact lens. In order to keep the patient’s confidence level high, a strong communication between the offices of the optometrist and the surgeon must be maintained. Dr. Smith suggests: “The optometry staff should visit the surgery center and go through the complete pre-op process, including lying under the laser, so they can personally experience what the patient sees. All of my staff has done this. It helps them understand how intimidating the procedure can be and allows them to better alleviate the fears of the patient.” Points to Remember:
Resource Contact Information In Office Edging and DrillingFor the practice that differentiates itself by service and revenue control, many incorporate a finishing lab that includes or makes preparation for the addition of drilling. Edging in-office is sophisticated and more automated. Advanced machine technology allows production of high quality eyewear while staff can improve their own abilities and skills. The default edger system is patternless using a frame tracer to digitize frame characteristics. Newer technology begs the questions: 1. Manual or automated lens layout and blocking? And 2. Drilling, and if so, manual or a drilling edger? Automated layout and blocking recognize the Rx and locate the optical center. Using a ‘xy’ table the device moves the lens to correct decentration, rotates the edging block to the correct axis and blocks the lens. Combined layout and blocking saves significant time, especially when staff is developing their own skills. Automated blocking uses the optics of SV, the outline of segmented multifocals and the inked markings of progressives for decentration and axis layout. (See Layout Blocker) Purchase considerations are: existing technician skill level, the comparison of machine cost vs. cost of a highly compensated optician doing lab work instead of selling. While many ECPs wonder if the cost of the machinery will pay for itself, the correct question is will the added capability allow my office to sell more of the higher value, higher margin products and therefore pay off the machine in less time than my numbers suggest now.
If the decision is to implement drilling i.e., the office is upgrading edgers or wants to be able to grow into drilling after implementing edging; the choice between a drilling edger and manual drilling station must be made.
Training should include knowledge of prescription analysis, the Boxing system, PD and decentration as well as machine operation. The tech must know when the device has done the job incorrectly. Implementation Drilling manually, but with a drill system that aligns the lens pair together is quickly implemented since the process is straightforward. The hardest part of rimless processing is assembly and alignment. This takes the right person and time to practice. Some rimless are easier than others and the practice should determine the steps needed to add designs to inventory. One can always send the more difficult jobs out to a specialty lab. Finishing the Screw for Drill Mount FramesWhen assembling three-piece drill mount frames, an elegant solution to the problem of loose or poor finishing of the screws and nuts is a reverse burnishing tool, available from AIT Industries.
As seen in the diagram, (See Top Clean) cut the screw off at the top of the nut. Cover the nut with the Top Clean and press down. The cutting tip “v” burnishes the remaining screw. The result is a brightly finished screw and the cutting helps keep the nut from getting loose. Resource Contact Information Benchmarking TechnologyConsider the practice that has implemented a variety of technologies. How would they know that they are deriving all the benefits they could expect and are patients getting all the services they want and need? Again, technology is a tool here to provide answers. The office backbone, the practice management system can deliver information through the report writer functions that tell how many, how much and how often. However, how do you know how that compares to the norms and the best in the industry?
The Independent Eyecare Professional Benchmark Analysis is an Internet-based financial simulation tool enabling the “Independent Eyecare Professional” (IEP) to quickly and simply benchmark many of the practice sales and operating aspects. With an extensive background as a CPA and as a financial consultant, Steve Wagner, a principal of C&E Vision developed the model from AOA and trade magazine statistics, from industry research and reports as well as personal interviews with professionals about their numbers. “The input matrix has many layers so the professional can add data to best understand the effects of large technology purchases, the effects of increased billings for procedures and product sales as a result of making patients better informed about health and eyecare options. The matrix allows a clear view of the effects of the private vs. insurance mix on a one office practice,” says Wagner. There are two versions of the IEP Benchmark analysis. The guest version has limited input variables, while the C&E Vision Services RewardsPlus member edition provides a substantial input matrix for numerous variables, including the relative percentage of the services performed, the pricing of these services and related direct costs. The graphs and data produced stress how good recall and inventory control can positively affect the P&L (Figure: Simulated P&L). How effective one is in using the marketing and inventory modules in a practice management software system can be measured when comparing to the average benchmarked practice. “The analysis is targeted at the $4- 500K with an average mix between private and managed care patients” said Wagner. “Just invest 30 minutes and areas that need more attention are easily recognized (Figures: Revenue and Cost of Goods).” For example, adding higher quality and/or branded products, that staff is trained to promote, helps enhance an office’s own brand and would increase revenue. A review of the revenue versus cost of sales would show how this could be done. In fact, with a benchmarking tool, a variety of what ifs are possible so that a clear set of goals and tactics can be developed. It also can show the how the insurance mix affects a practice (Figure: Per Patient Analysis). Technology can help assemble data into clear pictures and shorten the time needed to make changes and decisions in any business. Resource Contact Information |
December 2006
 The doctor prescribes solutions for healthy vision. That means that the eye exam and refractions that results in an Rx is not just a set of numbers but also a series of healthy sight recommended solutions. Using sophisticated technology to better discover, document and describe a patient’s condition makes a patient better informed and ultimately, may make the patient more compliant with the recommended treatments.
The doctor prescribes solutions for healthy vision. That means that the eye exam and refractions that results in an Rx is not just a set of numbers but also a series of healthy sight recommended solutions. Using sophisticated technology to better discover, document and describe a patient’s condition makes a patient better informed and ultimately, may make the patient more compliant with the recommended treatments.
 The inability to read chart notes can cause medical-legal issues and decrease efficiency in the clinic. The “cure” for this problem has historically been to hire a scribe, or “writer.” EMR software programs alleviate problems associated with poor penmanship. Pre-formatted letters are customized for the patient, save dictation and transcription time
The inability to read chart notes can cause medical-legal issues and decrease efficiency in the clinic. The “cure” for this problem has historically been to hire a scribe, or “writer.” EMR software programs alleviate problems associated with poor penmanship. Pre-formatted letters are customized for the patient, save dictation and transcription time As a result, modern-day offices are installing remote chart projectors. Remote projectors such as the MC-3 (Topcon), simulate an infinity projection, allowing for pretesting rooms as small as eight feet by nine feet. Remote chart projectors have the capability of storing many individual charts and are controlled with a small handheld unit, or linked to a refracting system.
As a result, modern-day offices are installing remote chart projectors. Remote projectors such as the MC-3 (Topcon), simulate an infinity projection, allowing for pretesting rooms as small as eight feet by nine feet. Remote chart projectors have the capability of storing many individual charts and are controlled with a small handheld unit, or linked to a refracting system. The ARK-530A offers a range of -30 D to +25 D. In addition to autorefraction and “K” readings, it can compare data from the Marco LM-1200 or LM-1000 auto-lensmeter to the auto-refraction data. In addition to a subjective refraction, the ARK-530A provides sagittal “K” readings with eccentricity values and a printout that illustrates myopia, hyperopia and astigmatism to be used in patient education.
The ARK-530A offers a range of -30 D to +25 D. In addition to autorefraction and “K” readings, it can compare data from the Marco LM-1200 or LM-1000 auto-lensmeter to the auto-refraction data. In addition to a subjective refraction, the ARK-530A provides sagittal “K” readings with eccentricity values and a printout that illustrates myopia, hyperopia and astigmatism to be used in patient education.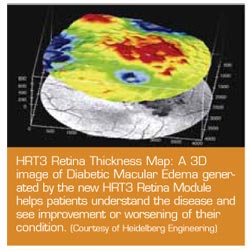 Involving the Staff in New Equipment Purchases
Involving the Staff in New Equipment Purchases Edging in office differentiates practices by service and flexibility. Buy the best that one can afford. In our opinion, only consider edgers that trace, edge, groove, and polish, have adjustable bevel and groove positioning, can control A and B lens shape sizing independently and work with all plastic lens materials. (See Drilling) The addition of drilling in office further adds to the opportunity for differentiation. Remember, rimless availability is the norm in almost all offices, how they are delivered differentiates offices.
Edging in office differentiates practices by service and flexibility. Buy the best that one can afford. In our opinion, only consider edgers that trace, edge, groove, and polish, have adjustable bevel and groove positioning, can control A and B lens shape sizing independently and work with all plastic lens materials. (See Drilling) The addition of drilling in office further adds to the opportunity for differentiation. Remember, rimless availability is the norm in almost all offices, how they are delivered differentiates offices. Return on Investment and cash flow are part of the decision and a simple calculator can show the months to recover the investment. An office that does eight drill jobs per day and pays an average $30/job can recover the costs of an automated blocker and drilling edger in less than 18 months just with the rimless work. Of course, this edger is used for all the other jobs. Each edger company can work through a ROI estimate with you.
Return on Investment and cash flow are part of the decision and a simple calculator can show the months to recover the investment. An office that does eight drill jobs per day and pays an average $30/job can recover the costs of an automated blocker and drilling edger in less than 18 months just with the rimless work. Of course, this edger is used for all the other jobs. Each edger company can work through a ROI estimate with you. A mechanically skilled employee is required for in-office edging and glazing. Math with signed numbers is essential. “Fine motor skills” are required for drill mount assembly and alignment. Lab techs must understand the quality requirements of the office and be able to see quality defects. Edger companies provide training during installation and on-going technical support.
A mechanically skilled employee is required for in-office edging and glazing. Math with signed numbers is essential. “Fine motor skills” are required for drill mount assembly and alignment. Lab techs must understand the quality requirements of the office and be able to see quality defects. Edger companies provide training during installation and on-going technical support. When adding the nut and tightening, the screw threads are cut and either a second cap nut is added or the screw is filed to be flush with the top of the nut. This can leave sharp edges that snag on the cleaning cloth or the length of the screw left is too long or not long enough for the cap nut. Here’s another solution.
When adding the nut and tightening, the screw threads are cut and either a second cap nut is added or the screw is filed to be flush with the top of the nut. This can leave sharp edges that snag on the cleaning cloth or the length of the screw left is too long or not long enough for the cap nut. Here’s another solution.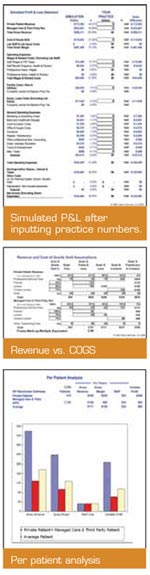 Consider participating in a management group (Williams Group for example) or with a consulting group (The Power Practice, Gary Gerber, OD) where their use of business analysis tools allows comparisons of your business to the norm and the range of practices within the group. If you are a member of the C&E Vision Buying Group, they now offer a new and very detailed Benchmark Analysis tool targeted at the independent eyecare, one office practice. If not a member, there is an abbreviated version anyone can try at www.cevision.com. C&E members can view vendor invoices on line as well as benchmark their business.
Consider participating in a management group (Williams Group for example) or with a consulting group (The Power Practice, Gary Gerber, OD) where their use of business analysis tools allows comparisons of your business to the norm and the range of practices within the group. If you are a member of the C&E Vision Buying Group, they now offer a new and very detailed Benchmark Analysis tool targeted at the independent eyecare, one office practice. If not a member, there is an abbreviated version anyone can try at www.cevision.com. C&E members can view vendor invoices on line as well as benchmark their business.






