
ANISOMETROPIA:
Treatment Starts Young
By Lori Passarelli, ABO-AC FNAO
Learning Objectives:
Upon completion of this program, the participant should be able to:
- Define anisometropia, its causes and symptoms.
- Gain an understanding of how aniseikonia affects binocular and Stereopsis vision and fusion.
- Design glasses for people with aniseikonia by changing lens properties.
Credit Statement:
This course is approved for one 1 hour O.D. CE credit by NYSSO
Faculty/Editorial Board
 Lori Passarelli ABO-AC FNAO
Lori Passarelli ABO-AC FNAO
Lori's father, an ophthalmologist, taught her to use the lensometer when she was 14, spawning a lifetime interest in optics and eye anatomy. Since 1998 Lori has managed the optical department at Orange Coast Eye Center, an ophthalmology practice in Fountain Valley, California. Lori is a lifelong learner with an affinity for physics and optics. She is passionate about helping patients select fabulous frames that make them feel good.
 In this course, we will
learn about the visual
and physiological effects
of anisometropia, the condition where the refractive
power between the two eyes is
unequal. We will discuss the
critical need for Anisometropia to be caught early in children to prevent the development of refractive amblyopia
that can lead to permanent
poor vision in the eye with the
strongest refractive error.
In this course, we will
learn about the visual
and physiological effects
of anisometropia, the condition where the refractive
power between the two eyes is
unequal. We will discuss the
critical need for Anisometropia to be caught early in children to prevent the development of refractive amblyopia
that can lead to permanent
poor vision in the eye with the
strongest refractive error.
When the difference is significant, other conditions develop such as Refractive Amblyopia, Aniseikonia and Anisophoria. We will also learn about designing Iseikonic lenses to decrease magnification differences between lenses.
What is Anisometropia?
Anisometropia is a difference in refractive power between the right and left eyes. The term is the derivative of the Greek root words: an = not, iso = same, metre = measure, ops = eye. Anisometropia is further categorized as Simple Hyperopic Anisometropia where one eye is emmetropic (normal) and the other hyperopic (farsighted); Compound Hyperopic Anisometropia where both eyes are hyperopic; or Simple Myopic Anisometropia where one eye is emmetropic and the other myopic (nearsighted); or Compound Myopic Anisometropia where both eyes are myopic; or Antimetropia where the eyes have opposite refractive power, meaning that one eye is hyperopic, and the other is myopic.
The discrepancy in refractive error resulting in Anisometropia causes problems because it is difficult for the brain to fuse the discordant image sizes refracted through lenses of dissimilar power. Technically, Anisometropia can mean any refractive difference, but people rarely suffer symptoms with less than 1 diopter of inequality.
It is estimated that 6 percent of those between ages 6 and 18 are affected with Anisometropia.
However, its pervasiveness is hard to pinpoint since refractive error testing can vary from doctor to doctor, and its definition is not consistently defined. If untreated, Anisometropia in children can result in amblyopia, a lifelong reduction in vision, as the brain suppresses the blurry image from the eye which can fail to develop correctly. For this reason, ODs and MDs diagnose and treat the condition early in life to ensure both eyes are used.
In clinical practice, Anisometropia is typically defined as having a refractive power difference of 2 diopters or more; however, as with any physiological condition, varying factors can influence the tolerance threshold to a larger or smaller degree. Most people with Anisometropia can fuse images with a variance below 3 diopters; however, incredibly, some people can integrate images with as much as a 6, 7 or even 8 diopter difference in lens power. Thus, the 3 diopter rule may be typical yet unreliable. The patient’s tolerance for the disparate refractive error may depend on several factors, including age, the type of Anisometropia indicated, symptomatology, the individual’s fusion capacity and spectacle history. For instance, a decades-long bespectacled person with a refractive difference of three diopters will probably be less bothered than an individual new to glasses. 1
The prognosis for Anisometropia depends not only on the refractive error but also on the type. People with hyperopia, for instance, report the most amount of trouble. Moreover, they may complain of symptoms of asthenopia or eyestrain. Eyestrain typically includes headaches around the eyes that may ensue as the person struggles to focus, causing eye muscle strain. Diplopia or double vision may also occur. The myopic anisometropic individual is typically free from asthenopia because they alternate fixation between their eyes, never fusing the dissimilar-sized images.
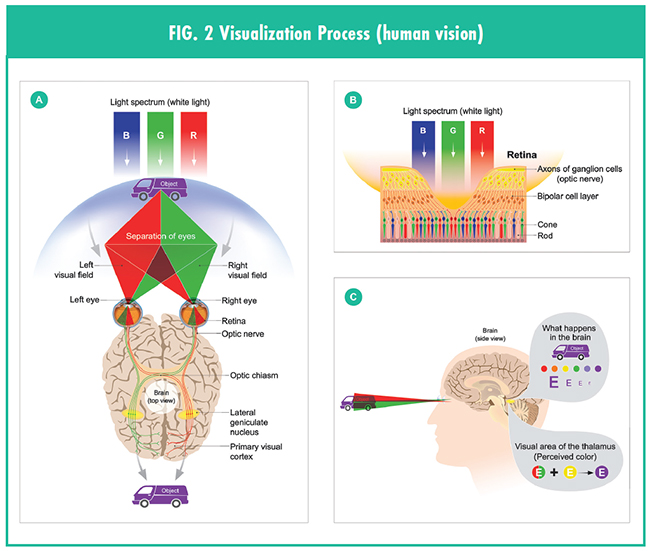
Binocular and Stereopsis vision: Binocular vision in Anisometropia is almost always limited or nonexistent. Using one eye at a time negates binocular vision, which hampers Stereopsis. Stereopsis affords us a 3D visual experience and happens because each eye sees an image from distinct angles. This is commonly referred to as horizontal disparities. Humans have forward-facing eyes separated laterally by approximately 3 inches on the head. The two images fall along the same visual axis, creating one image with depth and dimension. The visual cortex processes the disparities, and the result is binocular vision. Binocular vision orients us in space and helps us judge the nearness of objects. An easy experiment to test how each eye sees an object from varying vantage points is to hold an object such as a pen at arm’s length in front of your face and simultaneously close one eye at a time while staring at the pen. The pen shifts in space because the eyes see it from two angles. The dual images merge onto the fovea (central retina), creating a three-dimensional visual experience due to the distinct angles.
“When two eyes are employed, two additional factors play a role, the one not very important—namely, the act of convergence or divergence of the eyes—and the other very important—namely, the stereoscopic perception of depth by virtue of the dissimilarity of the images presented by a three-dimensional object, or array of objects, to the separate eyes.” (britannica.com/science/human-eye/the-perception-of-depth)
Stereopsis is a measure of binocular vision. When the eyes are working well together, we have good stereoscopic depth perception. Giashi, et al. studied the development of stereopsis and define fine and coarse stereopsis as follows: “Stereoscopic depth perception may be obtained from small retinal disparities that can be fused for single vision (fine stereopsis), but reliable depth information is also obtained from larger disparities that produce double vision (coarse stereopsis).” (doi.org/10.1016/j.visres.2013.07.011)
Reduced Stereopsis is prevalent in people who depend on one eye to see or have poor vision in one eye. This is especially true concerning fine Stereopsis, where both eyes must work together to achieve spatial detection.
Patients need good binocular vision and Stereopsis. However, when there is a disparity of more than 2D of power, the lenses inhibit fusion in the brain, impeding the 3D effect and depth perception. So, while corrective lenses improve visual acuity, when there is a 2 D or more difference between the two lenses, they cause fusion problems due to the unequal image size that each lens produces. We know that minus lenses minimize image size while plus powered lenses increase (magnify) image size. When one lens in a pair of glasses is plus and the other minus (Antimetropia), symptoms are highly likely, especially if the difference is 2 diopters of power or more. Antimetropia when refractive error is of opposite signs, one plus and one minus lens together are not the only factors in image size discrepancy. A high minus lens coupled with a low minus lens, of 2 diopters or more difference, may pose problems for the patient, disrupting binocularity, fusion and stereopsis.
Aniseikonia
When corrective lenses cause unequal image sizes, Aniseikonia is the result. Symptoms of Aniseikonia include headache around the eyes from eyestrain, dizziness, disorientation or distorted space perception, photophobia or light sensitivity, and nausea. After dispensing a pair of glasses to a patient, if they complain that the edges of paper or the door frame slopes, they may be experiencing disturbed spatial perception caused by Aniseikonia. A patient may also complain of the sensation of the floor rising or falling.
Aniseikonia derives its meaning from Greek, and its literal translation means unequal images. The difference in image size can result from the anatomical structure of the eyes or be induced by corrective lenses. The goal in designing glasses for Aniseikonia is to bring the disparate image sizes to an equal value. The typical tolerance threshold is a 3 to 5 percent inequality, but the threshold can vary as in Anisometropia. Moreover, opticians should consider symptoms of asthenopia on a case-by-case basis.
There are two types of Aniseikonia: static and dynamic. Dynamic Aniseikonia produces unequal image size during eye rotation. When looking through lenses of unequal power in the vertical or horizontal plane, induced prism occurs. This phenomenon is known as Anisophoria. Anisophoria is less problematic in the horizontal meridian than the vertical since the eye has naturally occurring horizontal reserves.2
The condition is most troubling for multifocal wearing individuals. The vertical imbalance may be problematic due to the prismatic imbalance when looking through the reading segment of a pair of spectacles if the power difference is more significant than 2 diopters. This imbalance can lead to diplopia. Remember, the perceived image moves away from the apex of the prism while the retinal image shifts toward the base. This results in image jump as the eyes shift their gaze toward the perceived image (apex of the prism) to align the base image with the fovea. Keep in mind when thinking of lens-induced phorias that no deviation occurs when the patient gazes straight through the lens. It is only when the eyes drop into the reading segment, typically 10 mm away from the optical center, that vertical prismatic imbalance occurs. If, for instance, the power in the right lens is +1.00 sphere and the left is +4.00 sphere, there is no prism when gazing straight ahead. However, the resulting vertical prismatic imbalance is 3 diopter difference as the eyes drop 10 mm to look through the reading segment. Bicentric grinding or slab off is one way to correct a vertical imbalance; however, for people with low adaptation, the easiest way to eliminate vertical imbalance is to order two pairs of glasses, one for reading and one for distance vision. Remember when considering a slab off, vision in both eyes must be sufficient; otherwise, the brain suppresses the weaker eye, whereby vertical imbalance is not an issue.
Static Aniseikonia produces unequal image size while the eyes are stationary. When a patient with static Aniseikonia looks at an object one eye at a time, the varying image size between the two eyes expresses as a percentage. If, for instance, Gloria sees an image that appears 5 percent larger in her right eye than her left, she is said to be experiencing 5 percent aniseikonia.
“Optically induced Aniseikonia results from Anisometropia and can be a factor in pseudophakia or after cataract extraction with an IOL implant in one eye. At the same time, the other one has not had the surgery or the corrected power is for monovision. Refractive lens surgery can also cause it if the final prescription of the two eyes is not equal. Aniseikonia of another type may result in retinal trauma such as compression or a stretched retina after surgery. The compressed or stretched retina employs more or fewer retinal receptor cells, making images larger or smaller than their actual size. Common retinal problems that may cause Aniseikonia are macular pucker, retinal detachment, edema, macular hole and retinoschisis, a condition in which the retina splits into two layers.” (opticaldiagnostics. com/info/aniseikonia.html)
An undesired but straightforward way to solve Aniseikonia is to cover one eye. No one is happy with this solution, and the good news is that as opticians, we can design glasses to help the patient without resorting to this archaic quick fix. For example, in Gloria’s case, we try to solve the problem by designing a left lens with more magnification, or a right one with reduced magnification, thereby changing the image sizes of each lens to balance them. Altering vertex distance, base curve, lens material and lens thickness can be deployed to this end. Of course, we know that contact lenses are the first choice to eliminate the effects of Aniseikonia since the lenses sit directly on the cornea and give a more natural visual experience to the person wearing them.
Axial and Refractive Ametropia
 When parallel light rays do not focus on
the retina during the eye’s relaxed nonaccommodated state, the condition is
called Ametropia. The result is myopia,
hyperopia or mixed astigmatism, or
hypermetropia. Ametropia is caused by
one of two factors, axial length (axial
Ametropia) or refractive Ametropia.
Refractive ametropia is caused by the eye’s
refractive curve components, including
the cornea, the crystalline lens, the tear
film and the vitreous. Knapp’s law applies
to axial Ametropia and states that an
object’s image size will be larger or smaller
than normal if the eye is too long or too
short, and that the spectacle lenses will
bring images to their actual size. In other
words, if the eyeball is too long, causing
myopia, the image size is more significant
compared to how an emmetropic or normal eye sees the same image.
When parallel light rays do not focus on
the retina during the eye’s relaxed nonaccommodated state, the condition is
called Ametropia. The result is myopia,
hyperopia or mixed astigmatism, or
hypermetropia. Ametropia is caused by
one of two factors, axial length (axial
Ametropia) or refractive Ametropia.
Refractive ametropia is caused by the eye’s
refractive curve components, including
the cornea, the crystalline lens, the tear
film and the vitreous. Knapp’s law applies
to axial Ametropia and states that an
object’s image size will be larger or smaller
than normal if the eye is too long or too
short, and that the spectacle lenses will
bring images to their actual size. In other
words, if the eyeball is too long, causing
myopia, the image size is more significant
compared to how an emmetropic or normal eye sees the same image.
According to Knapp’s Law, a corrected spectacle lens would reduce the size to normal, eliminating Aniseikonia. In practice, Knapp’s Rule fails for a few reasons; axial length rarely causes a refractive error on its own. Corneal curvature or other eye refractive properties usually play a role in manifestation. Secondly, astigmatic differences are always refractive by nature, and finally, optical lens shapes vary and thus produce different amounts of magnification. According to Knapp’s Law, spectacle lenses would remedy the disparate image sizes. However, as mentioned, contact lenses work better in clinical practice and should be the first choice in helping the patient. With that said, not everyone can wear contacts for one reason or another, and as opticians, we should understand the principles of optics in designing a set of spectacle lenses that will help the patient should this be the case. Changing the magnification properties of the optical lenses will reduce Aniseikonia and its symptoms.
The first step is to calculate the magnification produced by each lens and then determine if altering image size is needed for fusion. Spectacle magnification (Sm) compares image size seen through glasses to the uncorrected image size a person sees naturally. Its expression is a ratio such as 1.04 or 4 percent magnification or 0.96, or 4 percent minification. Remember, the typical tolerance for inequality is a 3 to 5 percent difference.
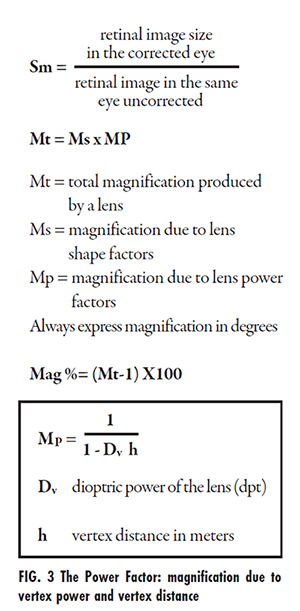
Power Factor and Shape Factor
When designing lenses, two factors come into play, the Shape Factor and the Power Factor, and the total magnification combines both of these elements. Magnification due to vertex power and vertex distance falls within the Power Factor, while the Shape Factor incorporates the base curve, center thickness and index of refraction. Altering one or more of these elements will influence the magnification percentage of the image projected on the retina. In other words, a person wearing a +5.00D lens will see a larger image wearing an 8 BC lens than a 5 BC lens. Likewise, increasing the vertex distance increases the image size in that same +5.00D lens.
The dioptric power, vertex distance, base curve, center thickness and lens material all work together to determine an ophthalmic lens’ magnification. Plus, powered lenses magnify images on the retina while negative lenses minimize them. The combination of the power and shape factors determine the total magnification of the lens.
The following rules apply when altering lens magnification:
• Steepen Base Curve: Increase magnification/decrease minification.
• Flatten BC: Decrease magnification/ increase minification.
• Increase thickness: Increase magnification/decrease minification.
• Decrease thickness: Decrease magnification/increase minification.
• Increase vertex: Plus, lens increase magnification/minus lens increase minification.
• Decrease vertex: Plus, lens decrease magnification/minus lens decreases minification.
When modifying a pair of spectacle lenses, the size of the final shape is irrelevant; what is more important is that the image size is more closely aligned—sometimes minimizing rather than magnifying the image of one eye benefits the cosmetic appeal of the spectacles.
While the formulas give you estimates of the changes needed, here are some general rules of thumb:
• For plus powered lenses: Choose a frame with minimal vertex distance and choose a small eye size.
• For the higher plus lens of the two lenses: Flatten the base curve, thin the lens and decrease the vertex distance by moving the lens bevel toward the front.
• For the lower plus lens: Steepen the BC, increase center thickness but do not exceed the thickness of the higher plus lens and move the bevel toward the back of the lens to increase vertex.
• For minus powered lenses: Choose a frame with minimal vertex distance, choose a small eye size.
• For the higher minus lens: Decrease vertex distance by moving the bevel forward, steepen the BC and increase the lens thickness.
• One lens plus and the other minus: Choose a small frame and choose a frame with a minimum vertex distance.
• For the plus lens: Flatten the BC, thin the lens and decrease vertex distance.
• For the minus lens: Decrease vertex distance and do not thin the lens.
For each 1 D change in BC, the vertex distance changes by approximately 0.6 mm. Magnification of images depends on the dioptric power of the lens and its vertex distance. If the vertex distance is changed, the following rules apply; a pluspowered lens moved further away from the eye increases the magnification, and a minus lens minimizes its size. Conversely, a lens sitting closer to the eye decreases the magnification of a plus lens and increases its size using a minus lens. Magnification from the shape (Ms) is dependent on the front curvature of the lens (D1) along with its center thickness (t). To use millimeters, divide by 10.
As the curve and thickness increases, so does the magnification. This is the shape factor. If altering the front curve to minimize or magnify, so must the back curve change to maintain the lens power; keep in mind these alterations affect vertex distance, and it too needs to be adjusted. A simple way to incorporate these principles is to use a high index for the higher plus lens and a regular index for the lower plus. Doing this alters thickness and base curve, and changes the back vertex distance.
Designing lenses that reduce Aniseikonia may seem intimidating or overwhelming when the patient flow is heavy, but the reward far exceeds the bamboozlement. After all, helping people see to the best ability possible is the goal of opticianry. Although we cannot modify the prescription prescribed by the doctor, we can alter magnification in each lens, thereby helping people gain fusion, binocularity and Stereopsis.