By Palmer R. Cook, OD
Many doctors find discussing eyewear is disconcerting, awkward and cause for an uncomfortable shift in the doctor/patient relationship. This only occurs if you, the doctor, make it uncomfortable. The patient has placed himself under your care. It’s your office. It’s your practice, and you are the one in charge. Your patient is eager to know everything you can tell him about his eyes, his health and his needs. With all of this in mind, why is it difficult to discuss what will best serve your patient’s needs? The following case history highlights how one doctor engaged his patient’s vision care needs and extended his mantle of care to include the needed eyewear.
PATIENT AND EYEWEAR CHARACTERISTICS
The patient was a 35-year-old man. His Rx is OD -4.50 -1.00 x 180, OS –4.00 -1.25 x 180, distance PDs are OD 30, OS 31. His old frame was a 52 o 18 with a 40 mm B measurement and a keyhole bridge. The old lenses were poly. The patient had a round, relatively large facial shape. The present frame showed excessive temple splay with the left temple more splayed than the right. The optical centers of the old lenses were placed 20 high (at the mounting line); this puts them 10 mm below the center of the pupils in the straight ahead position. The decentration for the old eyewear was 4 mm OD and 3 mm OS.
The patient was concerned about the weight and thickness of his glasses. His old Rx was OD -4.00 -0.75 x 003, OS -3.25 -1.00 x 180, and the lenses showed light curved scratches on front and back with deeper scratches on the back, near the upper and lower outer corners of each lens.
THE DOCTOR’S OBSERVATIONS
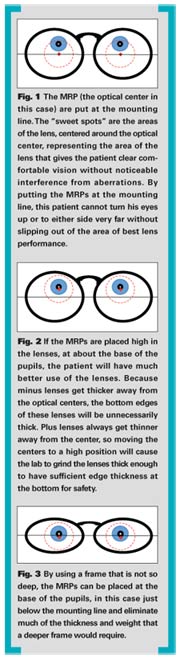
It was obvious to the doctor that using a wider adjustable bridge with a smaller eye size would give less lateral edge thickness. He could also see that turnback temples would widen the eyewear and help avoid the “splayed temples” appearance. A shortened B measurement would tend to lengthen his round face and make the lenses lighter. Using Trivex would also lighten the lenses and give him a larger “sweet spot” because of its higher Abbe value. By putting the optical centers higher, at the base of the pupils, the sweet spot would be more usable and most of the BU prism effect that he now experiences with his old eyewear could be eliminated. The doctor knows his optician will be able to recognize and correct all these issues. The eyewear portion of his consultation went like this:
“John, I noticed the scratches on your lenses. The lighter ones look like cleaning scratches. I want you to flush your new lenses with running water to remove grit before you use your lens cleaner, and I want you to be sure to only clean them as Judy, our optician, will explain to you. Some of the scratches also look like they were caused by using a clip-on of some kind. You are light sensitive, so I am recommending a photosensitive type lens that will adjust when you are in bright light conditions as well as prescription polarizing sun lenses for driving and to eliminate glare around snow, ice and water. Also, you are right-handed and I noticed that both temples flare outward too much on your old eyewear. Your left temple flares more than your right, so you may be removing your eyewear with just your right hand. Eventually this misaligns your frame and interferes with the way your lenses work, so you should use both hands when you take your glasses off.
“I will tell Judy to help you find a frame that will work well with the lighter lens material and will help your new prescription work better. I also want you to have lenses that will brighten your vision and reduce reflections. They are called AR lenses, and Judy will know what kind will work best for your prescription. As you may know, your new prescription will only work as well as the lenses that carry it.” (This doctor has a sign in his reception area, in his dispensary, and in his exam rooms and treatment rooms that says exactly that.)
“Before your prescription goes to the lab I will review the order to be sure that you will get the best benefit in comfort, vision and appearance.”
ANALYZING THE CONSULTATION
An analysis of the doctor’s brief eyewear discussion reveals how he kept the consultation on a doctor/patient level:
- He opened the discussion with comments about the old eyewear. This causes the patient to realize that his doctor does not limit himself to simply writing a lens prescription. Obviously the doctor’s expertise extends beyond examining eyes. Later the technician will probe what the patient particularly liked or didn’t like about the old eyewear. The answers could be very helpful in frame selection and in designing the new eyewear.
- The discussion moves to the issue of light sensitivity and the doctor’s recommendations for that sensitivity. He does not say exactly what type of photosensitive lens or prescription polarizing lens, because the final decision-making and explanation should be left to the optician. This doctor’s optician will let the patient know there are many types of photosensitive lenses and many types of polarizing lenses, and she knows what the doctor would want in the presenting situation.
- The doctor then returns to some issues and observations about the old frame. This doctor is clearly in “doctor mode,” not “salesperson mode.”
- The doctor indicates that he will be guiding the optician so she knows what is needed. In just three sentences he introduces the issues of frame shape, lens material and anti-reflective lenses.
- Finally, the doctor gives closure by indicating he will review the design of the eyewear before it goes to the lab.
- Had the patient asked about cost, the doctor might have answered, “Eyewear, frames and lenses together, in your prescription range start at about $______. I am recommending the best value for your vision. Judy can determine the cost exactly for you. Again, this response helps the doctor stay in the doctor/patient mode.
 REVIEWING THE ORDER
REVIEWING THE ORDER
When the doctor reviewed the order, he saw that the new daily wear frame was a 50 o 20 with a 30 mm B measurement. The new MRP heights were at 18 mm high. If the top of the frame was fitted at the same height as the old frame, this would put the MRPs at the base of the pupils. The new frame had turnback temples that added 5 mm of width to each side. The turnback design made the overall width of the new eyewear greater. The decentration had not increased but the distance from the OC to the lateral edge of each lens was 1 mm less in each eye. The new daily wear lenses were Transitions XtraActive with a top quality AR. The patient had also ordered DriveWear lenses by Younger Optics with an AR for the back surface only.
POINTS TO CONSIDER
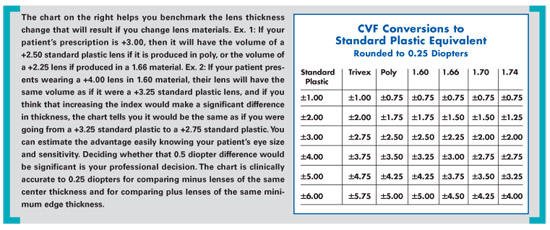
The lower index of the Trivex will not significantly thicken the new lenses. The difference will be about the same as if the power was about a quarter diopter greater (i.e., OD -4.75 and OS -4.00). The density of Trivex is less than poly, and that coupled with the reduced eye size and the reduced B measurement will make the finished lenses lighter.
The increased Abbe value will give less chromatic aberration and a larger sweet spot for more comfortable vision. The spread in power from red to blue light for a 4.5 diopter lens is 0.14 diopters for an Abbe of 32, and only 0.10 diopters for an Abbe of 45. This translates to a spread of 0.14 prism diopters in image displacement difference from red to blue for poly and only 0.1 prism diopters in image displacement difference for Trivex when the patient turns his line-of-sight just 1 cm from the optical center. The bottom line is that with a higher Abbe value, the patient can turn his eyes further from the optical centers while maintaining clear, comfortable vision. By raising the MRPs there will be fewer aberrations in straight ahead gaze, and the sweet spots of both lenses will be more usable.
Even though the patient did not do a lot of night driving, the doctor had refined his refraction under both high and low room illumination. The results with high illumination were: OD -4.50 -1.00 x 180, OS –4.00 -1.25 x 180, and this was prescribed for the daily wear glasses. Under low illumination the results were OD -4.75 -1.50 x 180, and OS –4.50 -1.75 x 180. This shift toward more myopia or less hyperopia in lower illumination is well-documented with patients who have active pupils. Because the patient had noticed a decrease in clarity at 20 feet with lower illumination, the doctor changed the Rx for the DriveWear lenses to OD -4.75 -1.25 x 180, and OS -4.50 -1.50 x 180. He told the optician to tell the patient that the prescriptions were slightly different between the daily wear eyewear and the lenses for driving because of his active pupils. He also told the optician if the patient decided to get full sunglasses for winter driving when the sun is low in the sky and for fishing, on the beach or around the pool, the full “low illumination” powers should be given in polarizing sun lenses with back surface AR.
You may or may not agree with all of the prescribing and design decisions given above, but you can bet the patient appreciated the level of care and attention he received. The doctor carefully addressed the eyewear issue without letting his post-exam consultation shift from a doctor/patient relationship to a buyer/seller relationship. Not only that, the doctor also clearly outlined what would work best for the patient, and he drew the optician into the interaction in a way that gave her authority and guidance. Most important of all, the doctor was involved throughout the patient’s vision care, and the patient received eyewear that incorporated all the needed and most up-to-date technology. ■
Palmer R. Cook, OD, is director of professional education at Diversified Ophthalmics, Cincinnati, Ohio.