

Protect, the Reason for Outdoor Eyewear
By John Lahr, O.D., FAAO and Mark Mattison-Shupnick, B.S., ABOM
Release Date: March, 2012
Expiration Date: March 15, 2017
Learning Objectives:
Upon completion of this course, the participant should be able to:
- Learn the most up-to-date effects of sunlight and radiation on the eye and adnexa.
- Understand why prevention used as a method to prescribe resonates with the consumer/patient.
- Understand the component parts of outdoor eyewear.
- Learn how to prescribe the right outdoor eyewear for all types of patients, i.e., adults, kids, seniors, general use, sports, etc.
Faculty/Editorial Board:
 Mark Mattison-Shupnick, ABOM is
currently director of education for
Jobson Medical
Information LLC, has
more than 40 years
of experience as an
optician, was senior
staff member of
SOLA International
and is a frequent lecturer and trainer.
Mark Mattison-Shupnick, ABOM is
currently director of education for
Jobson Medical
Information LLC, has
more than 40 years
of experience as an
optician, was senior
staff member of
SOLA International
and is a frequent lecturer and trainer.
 John Lahr, O.D., FAAO is vice president of provider relations and medical director of EyeMed Vision Care.
John Lahr, O.D., FAAO is vice president of provider relations and medical director of EyeMed Vision Care.
Credit Statement:
This course is approved for both ABO and NCLE credit.
This course is approved for one (1) hour of CE credit by the American Board of Opticianry (ABO). Course STWJM505-2.
This course is approved for one (1) hour of CE credit by the National Contact lens Examiners (NCLE). Course # CTWJMI335-1.
This course is approved for one (1) hour of CE credit by the Commission on Paraoptometric Certification (CPC).
This course his supported by an educational grant from LUXOTTICA
The sun nurtures our planet. It is the primary source of energy, heat and light. For centuries, cultures revered its presence and looked forward to its appearance every day as a reassurance that life would continue.
However, research about the sun and its energy in the form of radiation has also been shown to be problematic. While best understood by most Americans as sunburn and its cancer potential, ultraviolet radiation is less understood, and more importantly, less considered for its cumulative effects on the eye and its surrounding skin. More recently, the additional effects of high-energy visible radiation (blue light) and its causative links to age-related macular degeneration (AMD) add to the requirement for the right protective outdoor eyewear. There are three actionable ideas here, and they are: learning the latest information, protecting all patients and understanding the components of quality outdoor eyewear.
THE PROBLEM
In 2008, Review of Optometry reported that the U.S. was spending more than $50 billion a year on vision problems. As we've seen, the costs of medical care have continued to rise as well as the overall prevalence of eye disease. The National Institute of Heath estimates that more than 45 million Americans age 40 and over will be blind or visually impaired from AMD, glaucoma, diabetic retinopathy or cataracts by the year 2020. What does the sun have to do with it?
 The cumulative effects of ultraviolet radiation (UVR) have been implicated as a cause of cataracts, keratitis, pingueculae, pterygia, various eye and skin cancers, wrinkles, as well as age-related macular degeneration. However, UVR can also be good since it aids in production of vitamin D and its major source is exposure to the sun. Lack of sun exposure and vitamin D deficiency (a worldwide health problem) have been linked to many serious chronic diseases, including autoimmune, infectious and cardiovascular disorders, as well as cancers. Recent studies have suggested that the components of vitamin D production are beneficial as anticancer agents in the body. Though there is a contradiction here, we believe that with the right information about UV, every eyecare professional (ECP) can provide a balanced plan for every patient.
The cumulative effects of ultraviolet radiation (UVR) have been implicated as a cause of cataracts, keratitis, pingueculae, pterygia, various eye and skin cancers, wrinkles, as well as age-related macular degeneration. However, UVR can also be good since it aids in production of vitamin D and its major source is exposure to the sun. Lack of sun exposure and vitamin D deficiency (a worldwide health problem) have been linked to many serious chronic diseases, including autoimmune, infectious and cardiovascular disorders, as well as cancers. Recent studies have suggested that the components of vitamin D production are beneficial as anticancer agents in the body. Though there is a contradiction here, we believe that with the right information about UV, every eyecare professional (ECP) can provide a balanced plan for every patient.
High Energy Visible light (HEV), the wavelengths between 380 and 500 nm (blue light) have been implicated as a contributing cause of age-related macular degeneration. Blue light is part of the spectrum of colors we "see every day. Its accumulation affects the cone's ability to process light leading to possible oxidative damage, which can be irreversible in the retina.
UV and HEV are abundantly present outdoors. For outdoors, there's a plan—a quality pair of outdoor eyewear that absorbs UV and HEV. Dr. RW Young wrote: "Use of sunglasses that block all ultraviolet radiation and severely attenuate high-energy visible radiation will slow the pace of ocular deterioration and delay the onset of age-related disease, thereby reducing its prevalence. A 20-year delay would practically eliminate these diseases as significant causes of visual impairment in the United States. Today, it's estimated that one-fourth of the population has a significant cataract by age 75. Using Dr. Young's claim, that age would become 95. The overall visual health of the population would be transformed and the reduction in the costs of care could become part of the economy in a more positive way.
Concentrate on controlling the effects of UV and HEV where they appear the most threatening—outdoors. Protect with outdoor eyewear.
CLINICAL EVIDENCE
There's an ever-increasing body of evidence supporting the requirement to protect Americans from UV and HEV. Here, we discuss a variety of older and more recent research that when communicated, patients will agree outdoor eyewear is required.
 The Beaver Dam Eye Study (www. bdeyestudy.org) funded by the National Eye Institute is an ongoing study that collects information on the prevalence and incidence of age-related cataract, macular degeneration and diabetic retinopathy, which are all common eye diseases causing loss of vision in an aging population. The study was designed to discover (or
detect) causes of these conditions. Of importance to the ECP are:
The Beaver Dam Eye Study (www. bdeyestudy.org) funded by the National Eye Institute is an ongoing study that collects information on the prevalence and incidence of age-related cataract, macular degeneration and diabetic retinopathy, which are all common eye diseases causing loss of vision in an aging population. The study was designed to discover (or
detect) causes of these conditions. Of importance to the ECP are:
- Increased sun exposure in the teens and into the 30s revealed increased risk of developing early retinal changes that result in AMD.
- Men with higher levels of UVB exposure were 1.36 times more likely to develop cortical cataracts.
- Considering the interaction of other things people do that create eye issues. For example, male smokers were 3.3 times and female smokers were 2.5 times more likely to have exudative macular degeneration.
- Sun-sensitizing medications have an interactive effect. From the Journal of the American Medical Association, August 2010, "The lens of the eye develops from the same layer of tissue as the skin, and medication that increases the skin's response to the sun may modify the effect of sunlight exposure on the eye as well. The use of sun-sensitizing medications is increasing.
In 1988, about 800 fishermen (Chesapeake Bay Waterman Study) were profiled after having spent years on the water. Some wore no eye protection, and those had three times as many cataracts as those who wore sunglasses or a brimmed hat. Men with double the exposure to UVB had a 60 percent increased prevalence of cortical cataracts. In addition, over 80 percent in each age group over 30, revealed drusen, deposits in the retina, which can be indicative of early macular degeneration. And continued data analysis revealed a link between blue, visible light exposure and macular degeneration.
From a 2008 Yale University Medcast by Dr. David Leffell, called "Skin, Coping with the Sun and Aging, he reported that young users of tanning beds exhibited the skin textures and cancers of old age. The suggestion here is that excess UV exposure prematurely ages skin, true also for the tissue surrounding the eyes.
Other studies show there is more at risk from UV and other light exposure than just the lens and retina. Farmers exposed to UV had significant eyelid and conjunctival pathologies compared to controls those not exposed. People with light iris color have an especially increased risk of uveal melanoma with increased UV exposure. Overall, today there is a greater lifetime exposure to UV than earlier generations. That's because there is increased UV reaching the earth's surface, we live longer than previous generations and many Americans have increased their activities outdoors.
More recently, there was a surprise about what were the most at risk outdoor times for maximum UV exposure. For skin, risk is greatest from 10 a.m. to 2 p.m. But for the eyes and ocular surfaces, the risk is greatest from 8-10 a.m. and from 2-4 p.m. That's because the brows provide protection from overhead sun. So if removal of UV and HEV will reduce risks of early cataract and retinal damage, a recent paper by D. Sliney, Ph.D., suggests that due to geometry, wraparound sunglasses are essential. UV absorbing contact lenses may offer the best mode for filtering UV exposure of the crystalline lens and the limbus. And for those over 50, there is added value to remove HEV wavelengths.
 WHO'S AT RISK?
WHO'S AT RISK?
Should you only recommend UV absorbing lenses for prescription patients? Of course not; there's no reason to distinguish between an ametrope and an emmetrope. In fact, recommending a complete eye exam for those that visit your office for quality plano sunwear is also in order. The importance of a comprehensive eye exam is critical to assess eye health and better advise about the effects of UV and HEV.
Be especially aware of those that are more vulnerable to the effects of UV and HEV. They are kids, kids, kids, those taking certain medications, people living at high altitudes, participants in specific sports and once again, kids. Why have we listed kids so many times? Just think about the last trip to the beach, pool or the lake. You can see it now—mom and dad standing there in sunglasses with squinty "non-sunglassed kids in tow. This scene is repeated hundreds of times a day.
According to several studies, the average child receives approximately three times the annual UV dose of the average adult and up to 80 percent of lifetime exposure before age 20. In children under 10, the lens transmits 75 percent of the UV but only 10 percent in a 25-year-old. Long-term exposure to UV rays can result in major eye diseases such as cancer, cataracts and macular degeneration. Outdoors, ALL kids require sunwear.
 PROTECT, PROTECT, PROTECT
PROTECT, PROTECT, PROTECT
A plan to protect all patients is required. After all, good recommendations promote eye health. Excellence in vision care has correctly moved to include wellness, disease management and its effects on vision. However, for many ECPs, that message has not been consistently delivered or as yet, not appreciated for its seriousness. Consider a helicopter view of your office. How many sunglasses are there visible to patients when they visit? What printed and digital materials are visible to patients at reception? Eavesdrop on your own and others' conversations about the requirement for outdoor eyewear… What did you hear? The effects in particular of UV and HEV are as yet still misunderstood and/or underestimated by both the clinician and optician.
For the consumer, it has been well-documented that they better understand the effects of UV on their skin as evidenced by the number of cosmetic and sunscreen products sold annually as well as a general awareness of the SPF factor. However, that is not the case for eyes, i.e., few consumers realize that ocular surfaces are just like skin and affected by UV in much the same ways. In fact, it's worse since the damage is cumulative and the various transparencies of the structures to the various wavelengths of UV and HEV compound to create other conditions. It is critical to understand the maladies and diseases indicated by UV and HEV exposure completely.
It's important to address how well we can protect by delivering Outdoor Eyewear. Currently, we have not gone as far as we should as a profession and industry. Both prescription sunglass sales and photochromic lens sales as a sunglass substitute are still about one in five Rxs sold. That means about two-thirds of prescription eyeglass wearers haven't gotten the message that outdoor eye protection is critical. As we said, outdoor eyewear isn't just prescription sun. At the independent practices, the best offices do 20 percent and 10 percent of their gross revenue from Rx and plano outdoor eyewear respectively. In Part 2, PRESCRIBE, we'll detail the metrics to deliver quality outdoor eyewear and review actual current industry performance.
PROTECTIVE TOOLS
There are plenty of product tools designed to protect every American. In frames, it is a function of design and size; in lenses, protection from UV and HEV is derived from material and treatment. The following is a menu of ways to provide UV and HEV protection while adding style and fashion to every patient. When protecting, think UV is like water—if there's an opening, it will find it. "100 percent UV protective should now mean protection from UV: 1. Through the lens. 2. Around the side, and 3. Bouncing off the lens' surface. See the online version of this CE for more details.
Frames: Coverage is the operative term here. That doesn't necessarily mean big. We're looking for an outdoor frame whose inherent style fits close, matches the contours of the face and orbits and delivers style that makes a patient want to wear them. Wrap frames immediately come to mind and they are the recommended best solution since they will usually also prevent UV from entering the eye from the side. After all, a very dark lens can make the pupil dilate allowing UV side leak. Smaller flat sunwear may not provide complete protection.
 For sports frames, consider the field of view required for the sport as well as coverage. Lenses shaped with a "cheek cut provide a closer, more complete fit, as well as special nosepads for flatter
bridges. The same is true for kids. A soft nylon and wrap frame (with strap depending on age) is best. Be sure to control light leak.
For sports frames, consider the field of view required for the sport as well as coverage. Lenses shaped with a "cheek cut provide a closer, more complete fit, as well as special nosepads for flatter
bridges. The same is true for kids. A soft nylon and wrap frame (with strap depending on age) is best. Be sure to control light leak.
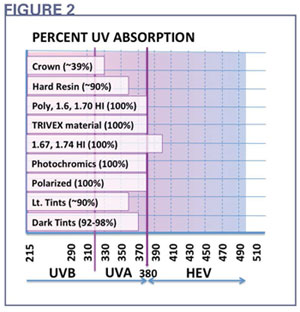
Lens Material: For 100 percent UV protection some lens materials inherently absorb all UV. Fig. 2 shows materials on the visible spectrum. Note that no material absorbs HEV, though the very high-index lenses automatically absorb to 400 nm.
How do you know a lens is 100 percent UV absorptive? For consumers that may just mean reading a label on the lens. However, that's not always proof. For the professional office, knowledge of material attributes using technical collateral from trusted manufacturers ensures that the products promised are actually delivered.
Understanding the protective attributes through the lens requires an understanding of selective absorption or the way a lens material transmits radiation and the visible spectrum by wavelength (a transmission curve). For example, an AR coated polycarbonate lens absorbs all wavelengths to 380 nm, the ANSI accepted UV limit (Fig. 2). With AR, the transmission quickly rises to over 97 percent of the visible light transmission (VLT).
In Fig. 2, note how the polycarbonate HEV brown lens effectively absorbs wavelengths (400-480 nm). This polycarbonate outdoor sun lens effectively absorbs all wavelengths to 400 nm and limits the transmission of a portion of the HEV. Compare it to a plastic lens tinted Gray 3. The tinted gray lens transmits more of the UV (radiation below 380 nm) and blue (wavelengths from 400 to 480 nm). Therefore, the smart choice would be one that limits HEV; but it is up to you. Learn how lenses selectively absorb radiation and definitively select lenses that always absorb UV and HEV. As you can see, ordinary tinted plastic doesn't do the job. Consider plastic lenses with UV enhancing dyes.
TREATMENTS
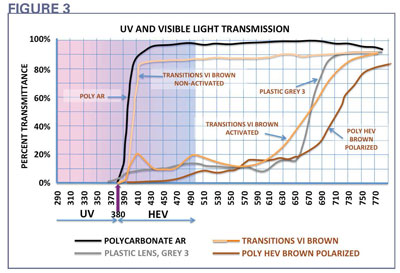 It's easy when it comes to polarized and photochromic lenses, as they absorb all the UV (Fig. 3). Here's the transmission curve of a premium brown photochromic lens with 100 percent absorption below 380 nm in the nonactivated as well as the activated form. Comfortably prescribe photochromics for the convenience of their variable tint as well as 100 percent UV absorption. As outdoor eyewear, the right colors and filtering characteristics are better. So when one pair of glasses must do for all, photochromics are ideal. Remember, the other obvious option is outdoor eye/sunwear. AR has not until recently affected the
transmission of UV. In fact, AR has typically been formulated to pass all UV through so as not to interrupt the ability of photochromic lenses to change. With the new Crizal series of lenses with UV absorbing technology, UV is now also absorbed on the lens back surface. As a result, this can prevent bounced UV from entering the eye when reflected off the back surface of the lens.
It's easy when it comes to polarized and photochromic lenses, as they absorb all the UV (Fig. 3). Here's the transmission curve of a premium brown photochromic lens with 100 percent absorption below 380 nm in the nonactivated as well as the activated form. Comfortably prescribe photochromics for the convenience of their variable tint as well as 100 percent UV absorption. As outdoor eyewear, the right colors and filtering characteristics are better. So when one pair of glasses must do for all, photochromics are ideal. Remember, the other obvious option is outdoor eye/sunwear. AR has not until recently affected the
transmission of UV. In fact, AR has typically been formulated to pass all UV through so as not to interrupt the ability of photochromic lenses to change. With the new Crizal series of lenses with UV absorbing technology, UV is now also absorbed on the lens back surface. As a result, this can prevent bounced UV from entering the eye when reflected off the back surface of the lens.
CONCLUSION
What can you do? Make PROTECT the actionable word in your office and talk to every patient about the issues that can result from too much UV and HEV. Remember, there is a body of evidence that the cumulative effects of UV and HEV contribute to a variety of eye issues that can create disabilities, blindness and costs many thousands of dollars. Opticians, optometric staff and prescribing doctors can help the American public understand the opportunity to protect their eyes starting with children through to seniors. For the doctor, translate the results of current research into simple terms, and then prescribe the right outdoor eyewear. For optometric staff and opticians, make the discussion a priority with the patient. Even if they can't get another pair of outdoor glasses, a seed has been planted. In this way, patients can make their own best choices about sunwear.

