
Vision's Declaration of Independence-Part One
UV, HEV and the Aging Eye
By Mark Mattison-Shupnick, ABOM, and John Lahr, OD
Release Date: July 1, 2013
Expiration Date: December 31, 2017
Learning Objectives:
Upon completion of this course, the participant should be able to:
- Understand the components of vision besides acuity.
- Learn the variety of age-related diseases and vision issues attributed to UV and HEV radiation effects.
- Know ways to prevent, treat and counsel patients about the effects of UV and HEV.
Faculty/Editorial Board:
 John Lahr, O.D., FAAO is vice president of provider relations and medical director of EyeMed Vision Care.
John Lahr, O.D., FAAO is vice president of provider relations and medical director of EyeMed Vision Care.
 Mark Mattison-Shupnick, ABOM is currently director of education for Jobson Medical Information LLC, has more than 40 years of experience as an optician, was senior staff member of SOLA International and is a frequent lecturer and trainer.
Mark Mattison-Shupnick, ABOM is currently director of education for Jobson Medical Information LLC, has more than 40 years of experience as an optician, was senior staff member of SOLA International and is a frequent lecturer and trainer.
Credit Statement:
This course is approved for one (1) hour of CE credit by the American Board of Opticianry (ABO). Course SJHI47
This course his supported by an educational grant from LUXOTTICA
 Independence, demanded by toddlers, tested by teens and coveted by seniors is significantly affected by vision. After all, independence is a part of each of our ability to earn a living, contribute to society and "drive at night." From a 1999 Canadian Social Trends survey (Catalogue No. 11-008), "The single greatest fear of most older people is that of becoming dependent. Although independence can take many different shapes and forms, for the 3.4 million Canadians age 65 or over, it often means having a car and being able to drive." It's no different in the U.S. How can the eyecare professional (ECP) contribute to sustaining a patient's good vision as they age, especially as an essential part of independence? One must understand the senior's vision, its components and the ways that eyewear can enhance it when needed.
Independence, demanded by toddlers, tested by teens and coveted by seniors is significantly affected by vision. After all, independence is a part of each of our ability to earn a living, contribute to society and "drive at night." From a 1999 Canadian Social Trends survey (Catalogue No. 11-008), "The single greatest fear of most older people is that of becoming dependent. Although independence can take many different shapes and forms, for the 3.4 million Canadians age 65 or over, it often means having a car and being able to drive." It's no different in the U.S. How can the eyecare professional (ECP) contribute to sustaining a patient's good vision as they age, especially as an essential part of independence? One must understand the senior's vision, its components and the ways that eyewear can enhance it when needed.
GOOD VISION
Vision is a sophisticated combination of acuity, the use of illumination, contrast and perception to see clearly. It is the conversion of all this visual information into an action or activity.
More specifically, acuity is the translation of objects seen and their details into sharp and crisp images. Contrast is the object in its surroundings where illumination, color and the environment can add or subtract from visibility and crispness. In the brain, the perceptive interpretation is the sum of all visual experiences, every time an object or objects are seen as either static or moving images. Add in the resulting depth perception from binocular vision, and vision becomes more than just acuity. As we age that changes. While experience and interpretative skills keep improving with use, changes to the eye and its structures affect acuity and contrast. That ultimately can affect vision and therefore, mobility and safety.
In this course, we'll investigate the effects of a lifetime of UV and HEV exposure on the human eye and vision. Until recently, there has been little action for the long-term out-door effects of UV and HEV. How can we say that when 85 percent of the U.S. population has sunglasses? In the U.S., not everyone has a quality pair of sunglasses nor understands the importance of protecting their eyes from ultraviolet (UV) rays and High Energy Visible (HEV) light outdoors. Second, only a small portion (about 6 percent) of the prescription-wearing public has quality prescription sunglasses.
Currently there are about 28 million cases of age-related eye diseases (cataracts, pterygia and age-related macular degeneration). By 2020, that number is estimated to become 43 million. If left untreated, these diseases will cause serious vision loss, blindness and significantly increase health and long-term care costs.
 WHO ARE THEY?
WHO ARE THEY?
In 2010, there were 40 million people age 65 and over in the United States, accounting for 13 percent of the total population. That older population in 2030 is projected to be 72 mil lion and representing nearly 20 percent of the total U.S. population.
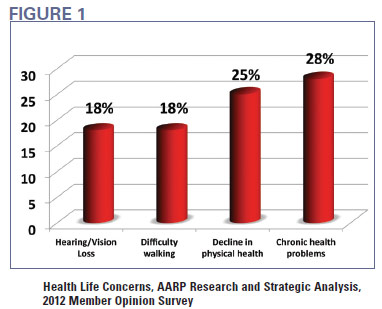
From an AARP 2012 member opinion survey (Research and Statistical Analysis), hearing and vision loss are part of the top four health life event concerns. Other facts include: The 75 and over age group spends twice as much for health care than the 55 to 64 group (15 percent of income vs. 8 percent). And in a recent review of life expectancy in 17 countries, U.S. men ranked lowest (age 75.6), and women ranked second lowest (age 80.7) attributed in part to the large number of uninsured without access to primary care, and unlike other countries with health care for all, violence is more lethal in the U.S.; and the U.S. has increasing populations with diabetes, heart disease and a higher infant mortality.
What does this have to do with UV and HEV radiation? UV and HEV are accumulated over a lifetime, and this population typically has not known that protecting their eyes is essential. Therefore, knowing the issues and the ways that quality outdoor eye-wear can help improve a senior's vision will help both your patients and your practice.
THE SENIOR, UV AND THEIR EYES
Acuity is the acuteness or clearness of vision, which is dependent on the sharpness of retinal focus. That means that the clarity of all of the ocular components and their media must transmit and receive light without issue. In an adult eye, the cornea and lens protect the retina from UVC (skin cancers), UVB (sunburn, blisters, skin cancers) and the UVA (skin aging). UVB and UVC are serious agents of skin tissue changes because the DNA directly absorbs them. The cornea and lens protect the retina by absorbing the greatest majority of radiation. As a result, only about 1 percent of UV and HEV can get to the retina. However, the effects are accumulated over a lifetime and become an issue for each of the senior's anatomical parts of the eye. Here's how.
Cornea: This transparent window is susceptible to sunburn just like the epithelial layer of the skin. Over a lifetime, corneal "sunburns" can be common from UVB overexposure, especially from reflection off surfaces like snow, water or even concrete. Artificial sources like welding arcs and UV tanning beds can also cause photo-keratitis. Treatment consists of mostly time to allow the epithelial layer to heal and replace itself. If severe, there might be patching, some sort of lubricant and lots of artificial tears to keep the surface lubricated. Recurring sunburn may result in longer-term problems.
 Treatment/Prevention (photokeratitis): 100 percent UV attenuating (absorbing and/or reflecting) sunwear in which the lenses provide complete coverage both from the front as well as the top and sides. Corneal sun protection is critical outdoors, especially when under extreme conditions like at high altitudes or at the beach or near the equator.
Treatment/Prevention (photokeratitis): 100 percent UV attenuating (absorbing and/or reflecting) sunwear in which the lenses provide complete coverage both from the front as well as the top and sides. Corneal sun protection is critical outdoors, especially when under extreme conditions like at high altitudes or at the beach or near the equator.
Other: The cornea loses its high sensitivity to touch in old age so may become more susceptible to damage. In some, a white ring develops in the periphery of the cornea called arcus senilis. Fading after birth, arcus senilis reappears later in life, often associated with cholesterol deposits. It is rare but the result of significant UV exposure is Climatic Droplet Keratopathy or an accumulation of deposits in the cornea's middle layer, the stroma. It can leave scars and affect sight overall.
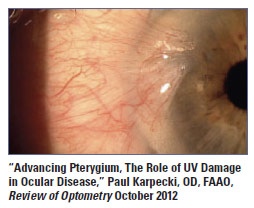
Sclera/Conjunctiva: Commonly attributed to UVA and UVB exposure (Chesapeake Bay Waterman Study), the nodule in the conjunctiva called a pinguecula results in a bump nasal and/or temporal of the limbus. It is often rich in blood vessels that fill to make the eye appear very bloodshot after being in the sun too long or outdoors in the wind where the surface of the eye gets dry.
Chronic sun exposure is also associated with pterygia, a wedge-shaped membrane or pinguecula crossing the limbus. If it grows close to or into the line of sight, the associated topographical shape changes make it necessary to remove it before there are dramatic vision changes. Unfortunately, pterygia reoccurs but newer techniques have been effective at halting the progression after surgery.
Treatment: 100 percent UV attenuating sun-wear; wrap eyewear is a distinct advantage.
Other: Squamous cell carcinomas of the cornea and conjunctiva are rare tumors. Know the warning signs of skin cancers.
Aqueous: From glaucoma.org: "Glaucoma can make eyes highly sensitive to light and glare, with some glaucoma medications exacerbating the problem even further. Sunglasses are an easy solution that makes life more comfortable when outdoors, while also providing critical protection from the sun's damaging ultraviolet (UV) rays."
Treatment/Prevention: "Glaucoma is a complicated disease in which damage to the optic nerve leads to progressive, irreversible vision loss. Glaucoma is the second leading cause of blindness." (glaucoma.org) Glaucoma patients are aided by quality sunwear that is 100 percent UV absorptive.
Crystalline Lens: The lens absorbs UV and depending on its yellowness, HEV radiation.
 The accumulated radiation effects are associated with cataracts and age-related macular degeneration. In a cataract (an opacity of the lens nucleus, cortex or capsule), lens cell proteins are changed by UV radiation. That results in a yellowing of the lens and a reduction of the light passed directly through the lens (opacification). Cortical cataracts, white triangular-shaped patches start at the lens edge. The most harmful to the lens is UVB. Over a lifetime, the condition gets worse requiring removal of the lens and an optical replacement by an intraocular lens (IOL), contact or spectacle lens or a combination of these.
The accumulated radiation effects are associated with cataracts and age-related macular degeneration. In a cataract (an opacity of the lens nucleus, cortex or capsule), lens cell proteins are changed by UV radiation. That results in a yellowing of the lens and a reduction of the light passed directly through the lens (opacification). Cortical cataracts, white triangular-shaped patches start at the lens edge. The most harmful to the lens is UVB. Over a lifetime, the condition gets worse requiring removal of the lens and an optical replacement by an intraocular lens (IOL), contact or spectacle lens or a combination of these.
"Cataract affects nearly 22 million Ameri-cans age 40 and older. By age 80, more than half of all Americans have a cataract. Direct medical costs for cataract treatment are estimated at $6.8 billion annually." ("Vision Problems in the U.S.: Prevalence of Adult Vision Impairment and Age-Related Eye Disease in America," Prevent Blindness America and the National Eye Institute, 2008)
Yellowing of the lens becomes apparent by puberty changing the amount of UVB that gets to the retina. But that means the lens is effectively transparent to UV in infants, toddlers and young children. The lens continues to yellow with age but a combination of genetics, diet, lifestyle and UV radiation causes some variability by the time we are seniors. A nuclear sclerotic or brunescent cataract is a lens that has become too dark yellow or brown, obstructs vision and requires removal.
This coloring of the lens also has implications to the way that colors are perceived. A brown lens absorbs the short wavelength blue light much like brown tints and polarized lenses. Color changes in the lens slowly change the appearance of the world we see, reducing the blue. As a result, when opticians deliver new glasses to a patient that has just had a very yellow to brown cataract removed and replaced by an IOL, they often hear from the patient, "Wow, that blue is so blue."
That's because they are again seeing all the visible spectrum of colors. The change of color sensitivity has less an effect on vision than does luminance or the amount of light. For the aged eye, that means the darkness of sun lenses for outdoor use requires some discussion with your patients.
Reading may become difficult for some nuclear cataract patients before removal is indicated since the opacity can alter the clarity and contrast of letters or images on a page.
Larger cylinder and axis changes in prescription or increased minus are often indicators that a cataract has begun to affect vision. The results may be noticed as increases in scatter or haze, or a subtle lack of clarity.
UVA in a lens also results in fluorescence when absorbed. Fluorescence produces scatter and haze, less noticed perhaps by a young eye but can reduce important vision in an older eye with a smaller pupil and cloudy media.
Treatment/Prevention: For cataract formation associated with the accumulation of UV radiation, UV attenuating spectacle or contact lenses, quality outdoor eyewear, UV absorbing IOLs. For reading problems with cataracts, SV reading glasses provide more reading area and should be used in addition to their general-purpose progressives.
 For the senior's reduction in color sensitivity, lens filter colors and polarization that do a good job to increase color contrast are the right choice. They are the typical browns, ambers and green. However, new lenses have been formulated to improve color contrast including gray. Anecdotally, when I take my senior customers outside to sample gray or brown sun lenses, they typically choose a brown polarized. The increase in contrast improves the edges and visibility of the things they see while the darkness of the lens adjusts the too-bright sunlight just the right amount for a variety of shadows, bright sun and daytime driving. They are also very comfortable to wear.
For the senior's reduction in color sensitivity, lens filter colors and polarization that do a good job to increase color contrast are the right choice. They are the typical browns, ambers and green. However, new lenses have been formulated to improve color contrast including gray. Anecdotally, when I take my senior customers outside to sample gray or brown sun lenses, they typically choose a brown polarized. The increase in contrast improves the edges and visibility of the things they see while the darkness of the lens adjusts the too-bright sunlight just the right amount for a variety of shadows, bright sun and daytime driving. They are also very comfortable to wear.
Vitreous: Floaters are probably the most common change to the vitreous noticed visually.
There is some evidence that UV has an effect on making the vitreous more liquid, with floaters becoming more numerous and contributing to a posterior vitreal detachment. A detached vitreous, i.e., when the vitreal membrane separates from the retina is common in the over 55. Patients will complain of a spider-like shadow. It may or may not be accompanied by flashes of light. Regardless, it should be checked by an eyecare professional.
Prevention/Treatment: There is usually no treatment for floaters other than assuring your customer that while they are normal, review by an eyecare professional is always recommended. The shadow that is noticed will also usually disappear as the eye/brain learns that the shadow is there and ignores it.
Retina: The retina is exquisitely sensitive to light. The rods are able to detect motion and assemble the visual scene with very little light for night vision while the cones provide exceptional clarity and colors when there is sufficient light. These structures are also terribly sensitive to the toxic effects of UV and HEV. While the cornea and lens protect the retina from this radiation, except as a child, excesses of both continually bombard our eyes. As a result, protection of the retina is required throughout life.
UV is implicated in age-related macular degeneration (AMD) due to high exposure to UV over a lifetime. AMD is the major cause of vision impairment in the over 50 group in the U.S., and its prevalence is expected to increase as the number of those over 60 increases. Newer research about the effects of HEV, in particular the wavelengths centered around 430 nm (±20 nm) also show that this blue light plays a role in the incidence and severity of AMD. In both cases, free radical damage to the cells of the retina by UV and HEV is suggested.
 While the aging retina is more susceptible to this damage, the yellowing of the lens and the absorption of some of the blue might help reduce blue light exposure. However, oxidative damage of the retina continues to occur with aging and its own protective mechanisms become less effective with age. Fluorescent phototoxic chromophores accumulate in the retina; blue light reacts with them, stops the regenerative process and kills the cells that nourish the cones. The result is a graying, then total loss of central vision.
While the aging retina is more susceptible to this damage, the yellowing of the lens and the absorption of some of the blue might help reduce blue light exposure. However, oxidative damage of the retina continues to occur with aging and its own protective mechanisms become less effective with age. Fluorescent phototoxic chromophores accumulate in the retina; blue light reacts with them, stops the regenerative process and kills the cells that nourish the cones. The result is a graying, then total loss of central vision.
Aphakes (post cataract, no IOL) and pseu-dophakes (post cataract, with IOL) should be protected from blue light since the crystalline lens' protective mechanism is absent.
Good UV/Bad UV: Good Blue/Bad Blue is a distinction also for retinal consideration since UV is important for the production of vitamin D, and the long wavelength blue is used to control circadian rhythm. As a result, vitamin D supplements may be recommended or up to 15 minutes daily in the sun wearing of course, a quality pair of sunglasses. The short wave blue (430 ±20 nm) is implicated in AMD while the longer wave to 500 nm is needed to help regulate sleep patterns.
Prevention/Treatment: Protect the retina from UV and short wavelength blue. That means wearing quality sunglasses outdoors and the use of the newer blue light attenuating indoor lenses. Know whether an older customer has had a cataract removed. Understand that the senior has other visual issues that affect your recommendations for lens color and darkness. Polarized lenses that enhance contrast also work well. Color contrast enhancing lenses also improve performance outdoors.
OTHER STRUCTURES AND CONSIDERATIONS
Pupil: While pupil size and the high school senior might suggest any variety of things (not discussed in this course), pupil size decreases (in light-adapted conditions) in the senior. The senior discussed in this course typically has a small pupil that does not get large even in dark conditions. One study from 1994 showed that a 20-year-old's pupil varies between about 2.5 mm to 8 mm while the 80-year-old's pupil changes from just under 3 mm to 4.5 mm under varying lighting conditions (Investigative Ophthalmology & Visual Science, March 1994, Vol. 35, No. 3).
The senior's smaller pupil and resulting lack of illumination in some situations can be a problem; they can't see an empty seat in the movies, have problems when driving in overcast conditions or at dusk or reading a menu in a restaurant. The lack of illumination from pupil size, when combined with a cloudy vitreous, cataract in progress and or retinal issues requires your counsel on the best eyewear for seniors.
Lids and Adnexa: Aging causes lid laxity (droopy lids), among other things. UVA penetrates deeply into the skin and contributes to these changes. A drooping lid can significantly reduce the visual field. If only one eye is affected, the patient may be uncomfortable because the vision between the two eyes is inconsistent.
 But the damage and cancers that UV is causative on the lids and adnexa are more serious. UVB and UVC are known carcinogens. UVC is mostly absorbed by the ozone layer but excess and accumulated UVB is the problem. It contributes to basal and squamous cell cancers as well as malignant melanomas.
But the damage and cancers that UV is causative on the lids and adnexa are more serious. UVB and UVC are known carcinogens. UVC is mostly absorbed by the ozone layer but excess and accumulated UVB is the problem. It contributes to basal and squamous cell cancers as well as malignant melanomas.
Prevention/Treatment: 100 percent UV attenuating outdoor eyewear, large enough and shaped properly to provide the right amount of coverage for the lids and surrounding skin. Of course, the proper use of hats and a high SPF sunscreen applied frequently is also necessary.
END OF PART ONE
Armed with knowledge of the effects of UV and HEV, what specifically should your advice be to customers? Part Two of this course describes a recommended plan for exam, lens performance, color vision considerations, driving advice and when corrections no longer make a difference, low vision tools for the visually impaired.