

Fitting the Very Young and Non-Verbal
By Danielle Crull, ABOM
Release Date: March 15, 2014
Expiration Date: September 27, 2018
Learning Objectives:
To update the ECP on changes and adoption practices for a lens material that is capable of being the overall lens platform including:
- Define the special fitting and adjusting needs of children who can't tell you themselves.
- Develop a method to identify and deliver well-fit and adjusted children's eyewear.
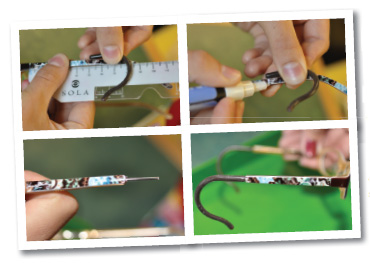
- Learn how to add and adjust a comfort cable to a standard but too long temple.
Faculty/Editorial Board:
 Danielle Crull, ABOC, owns A Child's Eyes, an independent optical store specializing in pediatrics in south central Pennsylvania. She became a Master Certified Optician in 1997, and her thesis topic concerned the differences between dispensing to children and adults. She lives in Dillsburg, Pa., with her husband and three children, all of whom work in her business.
Danielle Crull, ABOC, owns A Child's Eyes, an independent optical store specializing in pediatrics in south central Pennsylvania. She became a Master Certified Optician in 1997, and her thesis topic concerned the differences between dispensing to children and adults. She lives in Dillsburg, Pa., with her husband and three children, all of whom work in her business.
Credit Statement:
This course is approved for one (1) hour of CE credit by the American Board of Opticianry (ABO). Course SWJH536
 "The world is full of obvious things which
nobody by any chance ever observes." —Sherlock Holmes
"The world is full of obvious things which
nobody by any chance ever observes." —Sherlock Holmes
As an optician specializing exclusively in pediatrics for 15 years, I feel more like Sherlock Holmes than an optician. I have learned to be quite the investigator when fitting eyewear. My daughter, who is a certified optician, often stands by me as my Doctor Watson while we watch, assess, measure and fit the littlest ones without them ever even knowing it.
Because most of my patients are under 3 years old or are special needs and non-verbal, the optician's wornout question of "How does that feel?" doesn't work. How can we expect someone to know how it feels, when they don't know how it should feel? Instead of talking to the patient, I let the glasses speak for themselves. Any pair of glasses will tell you everything you need to know in about five to 10 minutes of careful observation. Or as Sherlock Holmes said, "It is a capital mistake to theorize in advance of the facts."
 The first step to a well-fit pair of glasses has nothing to do with fitting at all; it has to do with choosing. The question I ask myself when showing a first-time patient any frame is, "Does this frame fit?" which is followed closely by a second question, "Can it be modified to fit?" Every frame should be "pre-approved" by you as the optician. When trying glasses on your little patient, ask the above question and if it won't work, then hide the frame away. Let the parents choose only from the group of frames that will produce a good result.
The first step to a well-fit pair of glasses has nothing to do with fitting at all; it has to do with choosing. The question I ask myself when showing a first-time patient any frame is, "Does this frame fit?" which is followed closely by a second question, "Can it be modified to fit?" Every frame should be "pre-approved" by you as the optician. When trying glasses on your little patient, ask the above question and if it won't work, then hide the frame away. Let the parents choose only from the group of frames that will produce a good result.
So what should you do when the frames are the right size, but aren't exactly the right fit? That's where the second question follows hard after the first. "Can the frame be made to fit?" With children, every frame will likely need some modification, whether or not that means ordering a different temple length, changing nosepads or even adding cable adapters. Nearly every frame we dispense at A Child's Eyes is modified in some way, some extensively.
The good news is that companies which are serious about providing quality children's frames, like ClearVision's Dilli Dalli line, have many temple lengths available both with and without comfort cables. Looking for manufacturers that offer these options makes fitting much simpler. We like to do the Hokey Pokey test at our office. "Put your whole head in and shake it all about!" If you are dispensing to children, you better be comfortable with modifying frames.
So you've found a frame that the parents and child likes, and is in the right ballpark as far as size goes. What's next? The mysterious art of fitting. It's best to start front and center and work your way back to the ear. Look at the bridge. If it has nosepad arms, are the size and shape appropriate for the child's bridge? You may need to change them to small round pads if the child has a wide flat bridge or to a small oval if the bridge is more developed and narrow.
If there are no pad arms at all, and the frame has a molded saddle bridge, be certain that there is plenty of clearance for eyelashes. The curse of long, beautiful eyelashes discounts many plastic frames. Also, if the frame's bridge doesn't touch completely around her nose, then that frame is not a good choice.
Moving around to the sides of the head, we need to look at the overall frame width. It's absolutely crucial that the eyes center properly, both vertically and horizontally. A frame too large is going to make the lens thicker and heavier than they need to be. Conversely, a frame that is too small, where the eyes are set up too high in the frame, will encourage the child to look over the glasses rather than through them.
In addition, it's critical that the frames are not too tight on the sides of the head. They should only touch at the top of the ear and have a minimum amount of pressure on the sides of the child's head. If the child has a wide face and a narrow PD, you may need to look for frame fronts that have longer end pieces to relieve the pressure on the sides. Every child's head is still growing, and the little ones are growing quite rapidly, so any excessive pressure against the skull can make the child uncomfortable and can even interfere with the normal growing process. Specs4Us (specs4us.com) offers frames with fronts especially suited for children with Down's syndrome. Their frames have low bridges and long end pieces because those children often have wider heads.
 Working our way back on the frame, we need to look at temple length and style. Do we need to add cables? Is the frame available with cables on it? Is the frame available in different temple lengths?
Working our way back on the frame, we need to look at temple length and style. Do we need to add cables? Is the frame available with cables on it? Is the frame available in different temple lengths?
When it comes to actual children's heads, it always seems like the wider the head, the shorter the tem- ple length. This unfortunately defies frame manufacturers' conventional wisdom, which is to make temples longer as the size gets larger. When fit- ting children, if a stock frame has the right size frame front, the temples often end up being impossibly long. This is why frame modification is so important.
If the frame doesn't come with the size temples you need or comes without optional cable adapters, you may need to shorten the temples or add your own cable adapters. I recommend comfort cables for all young children and most especially for children of all ages in wheelchairs. If a child spends a great deal of time in a wheelchair, regular skull temples are knocked against the headrest, pushing the glasses forward and down the nose. Children who wear hearing aids also benefit from cable adapters because the adapter fits nicely behind the ear alongside the hearing aid.
The very young can be quite difficult when taking a pupillary distance measurement. Often pupillometers don't measure down to their small sizes. Trying to coax a little one to look into the pupillometer can bring back some bad memories from the doctor's visit. They will often cry and resist. Once they are crying, it's game over.
I suggest a simple game of peekaboo. We use a PD ruler that has windows so the child can look through and see you. This tends to make them comfortable, and who doesn't like peekaboo? Center the PD ruler on the child's bridge and cover one eye with your thumb. Do something crazy to get their attention—find the inner child in you. If you have a really shy child, try playing peekaboo with mom and dad first. This will likely make the child want to join in with the next round of fun.
 Next, if the doctor has prescribed bifocals, you will need to measure a segment height. Young children will need a lined bifocal, which should be fit to the center of the child's pupil. Don't worry; such a high bifocal will not interfere with the distance viewing because so much of the child's distance is above eye level. The child uses the bifocal for up-close vision, so a
high bifocal is essential.
Next, if the doctor has prescribed bifocals, you will need to measure a segment height. Young children will need a lined bifocal, which should be fit to the center of the child's pupil. Don't worry; such a high bifocal will not interfere with the distance viewing because so much of the child's distance is above eye level. The child uses the bifocal for up-close vision, so a
high bifocal is essential.
In addition, bifocals are often prescribed for accommodative esotropia (inability to keep eye alignment when looking up close). When measuring for a bifocal height in these cases, you MUST pre-adjust the bridge of the glasses and hold them in place. Get down to eye level and use a marking pen to dot up the pupil center on the demo lenses. If you don't preadjust the bridge, you will be remaking those lenses, guaranteed. Measure from the bottom of the lens to the dot, and you will have a proper bifocal height.
After the PD measurement, next up is a temple length measurement. Their glasses have to stay on and stay put not only for good vision, but also to prevent catastrophes like broken glasses that fell off and got tromped on in the ball pit at Chuck E. Cheese.
I will assume you know how to measure for a skull temple, but for a cable adapter it is a little more complicated. When measuring for the cable adapter fitting, we measure from the screw or bend on the temple to the furthest curve on the ear. Again you may need to find your inner child to get them to cooperate.
I hold the cable adapter against the temple with one hand and use a ruler to measure the length that corresponds to the edge of the adapter. Use your ruler to measure from the inside of the cable up the temple to the bend or the screw. Slide the cable up or down until you get to the right spot behind the ear and make a mark on the temple. This mark is where the cable will begin, but not where you cut the temple. You should cut the temple about 10 to 15 mm longer to start.
If you have a plastic-covered temple, cut at the mark only through the plastic overlay and remove the covering. You can get a snug fit by flattening the end of the metal and warming the temple end so the cable adapter can ease into the fitting. Finish up by cooling it off with water after the cable is on. I always secure the cable adapters with gel control super-glue, but not until the patient comes in for the final fitting.
Fitting cable adapters on a frame can be a bit challenging, but every optician can do it and should do it. Cable adapters can be bought from companies like Hilco or Vigor and are a must in any pediatric optician's toolbox.
 Once the frame is chosen and the measurements have been taken, the glasses can be fit with the lenses, and the real investigation begins. Have the patient put on their new glasses and wear them for a short period of time. Go for a full 10 minutes if you can. Have them play or go for a walk; if they're an adult, have them read a magazine. We have an iPad in our office and use it often for the little kiddos. You'd be surprised how comfortable they are with an iPad. There are many free apps that you can download for the kids to play.
Once the frame is chosen and the measurements have been taken, the glasses can be fit with the lenses, and the real investigation begins. Have the patient put on their new glasses and wear them for a short period of time. Go for a full 10 minutes if you can. Have them play or go for a walk; if they're an adult, have them read a magazine. We have an iPad in our office and use it often for the little kiddos. You'd be surprised how comfortable they are with an iPad. There are many free apps that you can download for the kids to play.
There is a point where everything looks good to our eye. The glasses are straight, the pressure is perfect on the sides of the head, and the temples are fit properly behind the ears. Don't be fooled by looks, though. It's not how they look; it's how they wear. Because children's bridges often develop asymmetrically, and their skin is soft and tender, any unequal or unbalanced weight on will cause discomfort. This discomfort WILL cause the child to take their glasses off and become noncompliant.
It is important to observe them while they are playing or reading. Your patient may be non-verbal but they certainly do communicate. Nothing like ripping off their glasses to let you know that something is wrong! Sometimes they will squish their nose up, poke at their ears, look over the glasses and rub their eyes—a whole host of behaviors.
I've had little ones move their glasses by contorting their faces into all sorts of shapes until the nosepads hit a comfortable spot. When they do this, I just go with it.
"So this is where you like the nosepads touching, huh?" No problem. If it's sitting lower on the nose, pull the pad arms down on the frame so the pads sit in the acceptable spot, but the frame still sits up higher. A verbal patient would just say, "These nosepads are uncomfortable here," but the non-verbal patient will simply do what they need to be comfortable, even if that means pushing the glasses down their nose or setting them on the floor.
If they start picking at their ear, take a look... does it pull tight or touch a spot on one side and not the other, which causes it to feel funny to them? If so, make the necessary adjustments. If they keep trying to rub their eyes or pull the glasses away from their face and then put them back, chances are good that their eyelashes are touching the back of the lenses.
Once they seem to be leaving the frames alone, wait about 10 minutes and then remove the glasses. There are six points of touch on any pair of glasses: each side of the nose if they have pad arms (or the entire bridge itself if it is a saddle bridge), the tops of each ear and the backs of each ear.
 Once the glasses have been worn for about 10 minutes, you can take them off, and you will likely see some sort of impressions left behind. These impressions are indicators of how the glasses will "wear" over a longer period of time. If a child is given glasses that are even a little uncomfortable, they will learn to associate their glasses with discomfort. They will push them away and cry at the very sight, choosing to see poorly over being uncomfortable.
Once the glasses have been worn for about 10 minutes, you can take them off, and you will likely see some sort of impressions left behind. These impressions are indicators of how the glasses will "wear" over a longer period of time. If a child is given glasses that are even a little uncomfortable, they will learn to associate their glasses with discomfort. They will push them away and cry at the very sight, choosing to see poorly over being uncomfortable.
Sensitive skin will mark quickly and look more pink or red than average, but the marks will still fade quickly if the glasses are adjusted properly.
A young child's bridge is not developed yet, so it is often soft and fleshy. You will likely see impressions left on the nose just from the sheer weight of the glasses alone. As long as the impressions are even and go away shortly after the glasses are off, then they are of no consequence. However, if you notice the marks are deeper or redder on one side, or unevenly shaped, then adjustments will be necessary. Re-adjust the glasses until the impressions are even and disappear quickly once the glasses are removed. This may make the pads appear quite uneven on the frame. Never fear; this is because children's bridges often develop asymmetrically.
Expect to see a light mark at the pressure point at the top of the ear. There needs to be weight distributed to the top of the ears in order for the glasses to stay on, but it should not leave a deep ridge on the child's head, just a light impression. Again, it is all about balance. Marks should be equal in size and darkness on both sides of the head. If you see a larger mark on one side of the glasses, try pulling the temple outward and re-evaluate.
Once adjusted properly on the bridge and the tops of the ears, then look behind the ears. When adjusting the temples for a skull temple or a comfort cable, it is all about distributing the weight evenly over the entire length touching behind the ear. If a ridge is left anywhere behind the ear, it is too tight and should be re-adjusted. I love comfort cables for fitting here.
There is one final critical step to adjusting frames: educating the parents. Let the parents know what to look for when the glasses get out of adjustment, so they know when to come back in to have them re-adjusted. Although it may seem obvious, they should know that glasses need to stay put and not slide down. Also, light marks on the nose are common, but should be symmetrical and go away shortly after the glasses are off. They should also be on the lookout for marks behind the ears. Let them know to come back in before things get so bad that the child starts removing the glasses to relieve the discomfort, or worse, Dad takes his own pliers to them.
Once you become an investigative optician, you will find this type of adjusting applies equally to all your patients. I often hear the wonderful words, "No one adjusts my glasses as comfortably as you do!" from my older, verbal patients, as well. There are a lot of beautiful frames out there, but if they are not fit properly, they just become beautiful headaches. As Sherlock Holmes said, "They say that genius is an infinite capacity for taking pains." By taking your time and examining closely for a few minutes with each patient, you will make lifelong, loyal customers.

