

When That Sore Eye Is Something Much Worse
By Erich Mack, ABOAC, LDO, NCLEC
Release Date: July 1, 2014
Expiration Date: May 6, 2019
Learning Objectives:
To update the ECP on changes and adoption practices for a lens material that is capable of being the overall lens platform including:
- Become familiar with some of the more serious eye infections.
- Learn how these eye infections are transmitted and affect patients.
- Know how to recognize "red flag" symptoms and how to handle these patients properly.
Faculty/Editorial Board:
Erich Mack, B.S., ABO, NCLE, is a certified Arizona licensed optician. At Visions Optique, he assists in practice management, training and brings his personal style to everyday opticianry and vision therapy responsibilities as well as creating new CE courses.
Credit Statement:
This course is approved for one (1) hour of CE credit by the American Board of Opticianry (ABO). Course STWJH100
1 hour of CE credit by the American Board of Opticianry ~ Valid for credit through May 6, 2019
Infections can be the most devastating and scary ocular emergencies we encounter. Infections come in many forms and can be bacterial, viral, fungal or parasitic. They strike their victim in a variety of ways and are indiscriminate. In this article, we will cover the worst five ranked in order based on my subjective opinion. To create a hierarchy, a subjective ranking of transmission, symptoms, treatment options and contagion will be used. It may be possible that some opticians may never encounter these infections but it is important to note that these patients are in crisis, and as opticians, it is important to recognize the warning signs and direct these patients to the right professional.
Transmission: Transmission methods can vary. Some infections are non-transmissible and score low where others transmit easily and therefore score high. Some invading organisms may live in your backyard plants or water sources, which also will score higher.
Symptoms: Symptoms vary with each type of infection. The symptoms are categorized by pain level and longevity, which will determine the score. For example, itching would score lower than a melting cornea (more about that later). A recurrent infection would score higher than an acute infection.
Treatments: Treatments make up the third scoring category. Multi-drug resistant infections would score higher than an infection treated by petroleum jelly. Some infections require a lifelong treatment plan, which score higher than a two-week antibiotic regimen.
Contagion: Finally, how contagious the infection is will be scored. Epidemic capability would score highest and non-contagious infections would score the lowest in this category.
The "fearsome five" are the worst five afflictions based on my rankings and starting from the last.
| Number 5: Pthiras Pubis (aka Crabs). The crab louse, also known as the pubic louse, is a tiny insect parasite that lives and breeds exclusively in thick, coarse human hairs. Due to their wide, flat bodies, they don't fit well in regular thin hair areas such as the scalp, although there exists a cousin louse that does indeed survive very well in the scalp. This cousin louse is the embarrassing lice that every grade school kid dreads. The coarse hair folliculaphilic crab louse (Pthiras Pubis) is found in the pubic and eyebrow/lashes in humans. |
TRANSMISSION
- Tiny insect parasites usually found in pubic areas.
- Transmission to the eye area is commonly through sexual intercourse.
- There can be non-sexual transmission via family and/or roommates sharing towels, clothes, beds or closets.
SYMPTOMS
- Localized intense itching due to hypersensitivity to crab saliva.
- The crabs feed exclusively on host blood four to five times per day.
- Excessive itching can cause corneal scratching and/or open wounds which can lead to secondary infections.
TREATMENT
- The parasites can only survive a short time away from the warmth and humidity of the human body.
- Successful treatment of the eye area includes applying petroleum jelly to the infected site twice a day for 10 days.
CONTAGIOUS
- The female crabs lay three eggs a day and sweeps over the host quickly.
- Direct contact with infected persons or infected items can transmit the crabs to others.
- Highly contagious to other humans due to high dwelling density.
RANKING
- Ranks as number five due to its low pain, damage levels and ease of treatment.
But it makes the list due to its highly contagious nature.
| Number 4: Adenovirus or viral conjunctivitis (aka viral pink eye) ranks fourth on our fearsome five list. Adenovirus actually consists of a family of virus strains called Adenoviridae. These medium-sized viruses infect a large range of animals and cause a variety of illnesses. For our purposes, we will focus on the notorious pink eye, specifically viral pink eye. |
TRANSMISSION
- An Adenovirus is spread easily by accidental inoculation to others via sharing towels, shaking hands, coughing and public swimming pools. This is certainly a red flag for an optician to be aware of, you don't want to accidentally let your patient infect you.
- We all have had the unwitting pink-eye patient walk in and touch the check-in desk, try on glasses and generally inoculate the whole optical department. Be aware of the following symptoms.
 SYMPTOMS
SYMPTOMS
- Adenovirus causes intense itchy eyes and usually the eyes are crusted shut after sleep.
- Eyes tear excessively and have a red appearance and giant papillary conjunctivitis (GPC) is present under the lids.
- Puss-like, ropey discharge is often noticed with adenovirus.
- Painful photophobia can also occur in some patients.
- In rare cases, patients may be susceptible to a secondary bacterial infection which leads to a very painful and difficult to treat super infection.
TREATMENT
- Adenovirus usually can resolve itself within two to four weeks.
- There are support treatments to help alleviate the symptoms and prevent bacterial super infection.
- Cold compress, artificial tears and NSAID pain relievers are also commonly prescribed.
CONTAGIOUS
- Adenovirus is the most contagious of the fearsome five ocular infections.
- It is extremely contagious, and as with most viruses, it is very durable inside and outside the human body.
- It is so contagious that it can cause epidemics of the infection, called epidemic keratocon-junctivis (EKC), which are tracked by the Centers for Disease Control.
RANKING
- Adenovirus ranks at number 4 due to its extremely contagious nature, even reaching epidemic levels.
- The pain is high and the symptoms are extremely unpleasant but damage levels are low. However, it is short-lived and manageable.
| Number 3: Herpes Zoster Ophthalmicus (aka Zoster) weighs in at a strong third on the fearsome five list. Zoster is caused by the virus varicellazoster. It is the same virus we love to hate that causes chickenpox and the painful shingles disease. It should be noted that Zoster is not the same virus that causes genital herpes, and therefore it is not sexually transmitted. Zoster outbreaks occur when the virus, which lives around nerve fibers, decides to replicate and/or move to another body part. This outbreak is very unpleasant in appearance and usually strikes when the victim has a weakened immune system. |  |
TRANSMISSION
- Since Zoster is a second unique type of outbreak from chickenpox, it isn't directly transmittable.
- Only someone who never had chickenpox or a chickenpox vaccine would be susceptible. A person would need to have an open wound come in direct contact with a victim's Zoster outbreak. Even then only the chickenpox virus is transmitted with no guarantee of getting a Zoster outbreak.
SYMPTOMS
- Zoster is a very painful condition since it directly attacks sensory nerves and can last for weeks, months and sometimes years. Hospitalization is considered for some patients.
- The severe pain is spread around the eyes and the side of the face. The pain continues to persist for several days after the visible signs have disappeared.
- A very unpleasant-looking rash appears on the eyes, forehead and sometimes nose.
- It causes open wounds and when a crust forms, called crusting, the outbreak is beginning to resolve itself.
- Swelling and cloudiness of the cornea occurs during the outbreak as well as an increased intraocular pressure (IOP).
TREATMENT
- Zoster is a virus and antibiotics are useless.
- There are some antiviral eye drops, and pills that may shorten outbreak length but they must be administered as soon as possible (72 hours).
CONTAGIOUS
- Zoster is not directly contagious, it's the least dangerous for public contamination of the fearsome five.
RANKING
- Zoster is number 3 due to its extreme pain level and long-term effects. The physical symptoms are extreme as well. It is difficult to treat, and all treatments must start quickly to have any effect. Zoster scores low in the contagion factor as it does not spread from person to person, and there is no guarantee of an outbreak even if you are infected.
| Number 2: The terrifying infection by Pseudomonas (aka The Cornea Melter) is number two on the fearsome five list—and for good reason. Pseudomonas is a ubiquitous bacteria that is commonly found in soil, water and plants. Normally Pseudomonas is harmless to humans, however in certain situations, an extremely dangerous and nightmarish infection can occur. To add to the risk factor, all non-disposable contact lens wearers are at the most risk for a Pseudomonas infection. | 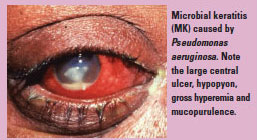 |
TRANSMISSION
- Pseudomonas is ubiquitous, and you probably have a few of the bacteria on you as you read this. However, the danger occurs when it forms a colony in the solution or case of contact lens wearer.
- A person that decides to create their own saline solution for contacts runs at risk of Pseudomonas infection since Pseudomonas is found naturally in water. Also if the saline solution isn't fully sterilized, Pseudomonas can thrive.
- A person that doesn't follow cleaning protocol in regards to their contact lens case is also at risk of allowing Pseudomonas to grow inside the case.
SYMPTOMS
- Pseudomonas infection to the eyes is devastating, often resulting in a melted cornea.
Thus the moniker "The Cornea Melter." - The infection is extremely painful due to nerve exposure associated with the melting of the epithelial and stromal cell layers.
- The wound is also susceptible to secondary super infection.
- If the Pseudomonas infection is not treated properly, and even in some cases of quick medical intervention, the victim's infected eye has to be removed (enucleated).
- If the infection is successfully stopped, often severe vision loss occurs. Severe being equated to no light perception (NLP), or 5/200 VA.
TREATMENT
- There are no vaccines for Pseudomonas, and it is notoriously resistant to antibiotics.
- Even if diagnosed and treated on day one of the infection, outcomes are grim, resulting in blindness or enucleation.
- With such a narrow window of treatment, finding an effective antibiotic is very challenging.
- Most often the only successful method is removing the infected tissue.
CONTAGIOUS
- Since Pseudomonas is usually harmless, it is not very contagious.
- The transmission vehicle is dirty contact lens solution and cases, so avoiding and disposing of them will eliminate any cross-contamination.
RANKING
- Pseudomonas is a close number 2.
- It ranks high because it is extremely painful and has horrifying corneal melting symptoms. It also ranks high due to its grim outcomes, even after immediate treatment, often resulting in loss of an eye or total blindness.
It is not very easy to contract except for noncompliant contact lens wearers and is uncommon so it scores low in that area.
| Number 1: The near invincible Acanthamoeba tops off the list as the infamous number 1. Like Pseudomonas, Acanthameoba is a microorganism that is ubiquitous. It is found in soil, water and many other everyday locales. Infection is rare, similar to Pseudomonas, but when infection does occur, it is extremely dangerous and devastating. And thanks to some high profile cases involving corporate quality control negligence, it edges out Pseudomonas in the list. It is a true free-living monster that can infiltrate and lay waste to a victim's cornea. | 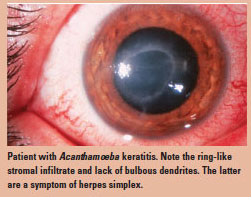 |
TRANSMISSION
- Acanthameoba is a very tough organism to kill as it can transform itself into a cyst.
- While in this dormant defensive form, it becomes resistant to temperature changes, pH changes and resistant to immune system attacks.
- The transmission vehicle is identical to Pseudomonas. Contact lens wearers are the main target for ocular Acanthameoba infection. People with recent agricultural inflicted eye trauma would be the second most common victims.
- A person that decides to create his or her own saline solution for contacts runs a risk of Acanthameoba infection. Since Acanthameoba is found naturally in water, if the saline solution isn't fully sterilized, Acanthameoba can thrive.
- A person who doesn't follow cleaning protocol in regard to their contact lens case is also at risk of allowing Acanthameoba to growing inside the case.
- Contaminated commercial contact lens solution can also cause Acanthameoba infection.
- In 2006, Bausch & Lomb recalled its contact lens solution due to Acanthameoba contamination. Also, a 2007 recall occurred for the same reason by the AMO corporation.
SYMPTOMS
- Initial symptoms appear as epithelial irregularities and ring-shaped infiltrates which mimic other much more common ocular problems. This makes it difficult to diagnose.
- A clue to Acanthameoba presence is an extraordinary amount of pain in what appears to be a minor low pain corneal problem.
- Exquisitely high photophobia is another symptom. People often come to their exam with two pairs of sunglasses on and a jacket pulled over their head to block out light.
- Super infection with bacteria is common, making treatment and diagnosis even more difficult.
- Damage to the cornea is severe, leading to total vision loss and/or corneal transplant.
TREATMENT
- There are no FDA-approved medications for treating Acanthameoba infection.
- Aggressive surgical and antimicrobial treatments need to occur immediately.
Even then the treatments last from three months to over a year with grim outcomes. Many patients still end up requiring corneal transplants. - Treatment with high levels of steroids is common; however, it often then leads to super infection with bacteria further complicating the problem.
- When Acanthameoba forms a cyst, it is nearly impossible to kill.
CONTAGIOUS
- Like Pseudomonas, Acanthameoba is not directly contagious.
- Sharing contaminated products like solution and/or cases can spread the infection.
RANKING
- Acanthameoba is number 1 in the fearsome five. It ranks high due to its extreme pain, damage and photophobia. It also is nearly impossible to treat and requires immediate aggressive surgeries. Even so, the aggressive treatments continue for up to over a year with grim outcomes, often resulting in corneal destruction and transplants.
Acanthameoba ranks high for its extreme toughness. However, it ranks low in the contagious area, as it is usually limited to contaminated contact lens solution and cases or agricultural caused eye injuries. It edges out Pseudomonas in this area due to the high profile contaminated product recalls.
What can an optician do when faced with the infected patient? It is important to recognize red flag symptoms. Recognition is important in order for precautionary measures to happen. Of course, every patient must be treated with the utmost respect and professionalism. Keep in mind the protocols of HIPAA and patient treatment when the patient is in the exam room with the doctor. Never speak ill of a patient or discuss the patient's conditions in front of other patients/customers. After the patient has left, have a discussion with the doctor about biohazard disinfection.
It is important to be aware of the fearsome five and other infections to which your patients can fall victim. Having knowledge of these ocular infection emergencies can be an indication of your office professionalism and make your patient/customers feel that they are in good hands. As opticians, we of course do not treat these patients, but having the basic knowledge can help you help a walk-in case and avoid giving poor advice. Parents that have their children go through contact lens training will certainly appreciate the preventative care training. Pseudomonas and Acanthameoba are great examples of how an optician can help keep their patients healthy. Proper education of contact cleaning protocols, replacement schedule or recommending daily disposables all help reduce Pseudomonas and Acan-thameoba infection risk. After all, giving sound preventative advice is giving superior care to your customers.

